



Cindy L. O�Bryant, PharmD, BCOP
http://www.ucdenver.edu/academics/colleges/pharmacy/Departments/ClinicalPharmacy/DOCPFaculty/H-P/Pages/OBryantCindyPharmD.aspx
Celexa dosages: 40 mg, 20 mg, 10 mg
Celexa packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

However medications54583 40 mg celexa buy with visa, the higher-dose group had better relief of dyspnea and more fluid and weight loss than the lower-dose group; 23% of the high-dose group had a significant deterioration in renal function, but at 60 days there was no difference in renal function between the two groups. However, in one retrospective analysis using propensity matching, hospital mortality was not different between low-dose and high-dose diuretic groups. This is seen in approximately one-third of hospitalizations for acute heart failure. These patients have longer hospital stays and higher readmission and mortality rates. The best treatment strategy for these patients is not clear, as patients with significant renal impairment have generally been excluded from large randomized pharmacologic heart failure trials. With chronic loop diuretic use, there is an increase in sodium reabsorption in the distal nephron and stimulation of aldosterone release. With renal dysfunction there may be reduced levels of drug delivered to the renal tubule. Diuretics that act distally in the renal tubule, such as metolazone or hydrochlorothiazide, or aldosterone blockers such as spironolactone, can be added. Combination diuretic therapy induces a greater diuresis than simply increasing the dose of loop diuretic further. Combining diuretics often augments diuresis even in the setting of significant chronic kidney disease, and a good response can be expected in more than 70% of patients. Particular attention must be given to monitoring renal function and electrolytes when combination diuretic therapy is prescribed61 (Table 27. Vasopressin Inhibitors the use of vasopressin inhibitors has been evaluated in clinical trials of treatment of acute heart failure. It acts through V1a receptors in vascular smooth muscle and myocardium, leading to peripheral and coronary vasoconstriction, myocyte hypertrophy, and positive inotropy. Vasopressin also acts through V2 receptors at the renal tubule collecting ducts to cause free water retention and hyponatremia. Levels of vasopressin are increased in patients with chronic heart failure, and higher vasopressin levels correlate with worse heart failure severity. Vasopressin release is stimulated by changes in serum osmolality and cardiac output and leads to further vasoconstriction and retention of free water. In contrast to loop diuretics, inhibition of vasopressin theoretically would not cause hypotension or neurohormonal activation and would not aggravate cardiac arrhythmias owing to electrolyte depletion. These medications increase urine volume and free water excretion, with a rise in the serum sodium concentration. There were no adverse consequences on heart rate, blood pressure, or serum electrolytes and there was more rapid improvement in dyspnea and signs of heart failure compared with usual therapy. A course of therapy with tolvaptan should not exceed 30 days, and its use is contraindicated in patients with significant liver disease. There is limited controlled trial evidence on which to base recommendations for their use. A retrospective analysis of unadjusted and propensity-matched data studied in-hospital mortality related to use of vasodilators.
Epidemic bloodstream infections from hemodynamic pressure monitoring: signs of the times treatment under eye bags 40 mg celexa purchase mastercard. Pseudomonas cepacia peritonitis associated with contamination of automatic peritoneal dialysis machines. Nosocomial infections from contaminated endoscopes: a flawed automated endoscope washer. An outbreak of Pseudomonas aeruginosa infections associated with flexible bronchoscopes. Risk factors for pneumonia and fatality in patients receiving continuous mechanical ventilation. Infections caused by intravascular devices used for infusion therapy: Pathogenesis, prevention and management. Risk factors for nosocomial candidemia: a case-control study in adults without leukemia. Candidemia in a tertiary care hospital: epidemiology, risk factors, and predictors of mortality. Hospital infection control: recent progress and opportunities under prospective payment. The financial incentive for hospitals to prevent nosocomial infections under the prospective payment system. Building and Validating a Computerized Algorithm for Surveillance of Ventilator-Associated Events. Infection control: the premier quality assessment program in United States hospitals. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings, 2005. Diagnosis, prevention, and treatment of catheterassociated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Are United States hospitals following national guidelines for the analysis and presentation of cumulative antimicrobial susceptibility data Analysis and presentation of cumulative antimicrobial susceptibility data (antibiograms): substantial variability across medical centers in the United States. Analysis and Presentation of Cumulative Antimicrobial Susceptibility Test Data: Approved Standard. Implementing antibiotic practice guidelines through computer-assisted decision support: clinical and financial outcomes. Impact of a computerized clinical decision support system on reducing inappropriate antimicrobial use: a randomized controlled trial. Rapid detection and identification of bacterial pathogens using novel molecular technologies: infection control and beyond. New microbiological techniques for the diagnosis of invasive mycoses caused by filamentous fungi.
However symptoms sinus infection order celexa 40 mg, before evaluating physiologic causes, it is important to rule out iatrogenic causes of hypotension including increased rates of medications that cause hypotension, such as analgesics, sedatives, or vasodilators. Vasopressors that support the blood pressure may have run out, been mixed at the wrong concentration, or disconnected from the patient may be another source of hemodynamic instability. Faulty monitoring, such as an improperly calibrated arterial line or height of arterial transducer relative to the patient, can also cause false indicators of hypotension. Similar to hypotension, iatrogenic causes of hypertension-such as inadequate sedation or pain control, hypothermia, increased or incorrect dosing, concentration of vasoconstrictors, arterial monitoring transduction positioning, and calibration errors-are also common and must be ruled out. Other important causes include increased sympathetic tone, hypertrophic left ventricle, and preexisting history of hypertension or stroke. In many cases, a nitroglycerine infusion is sufficient to treat postoperative hypertension. Secondary agents are typically determined by the surgeon or by institutional preference. In general, to protect suture lines, surgeons prefer to err on the side of lower blood pressure, particularly in the first few hours postoperatively, although this may compromise renal perfusion in patients who are hypertensive at baseline. By contrast, heated intravenous fluids and heated ventilator circuits can be used to prevent worsening hypothermia, but they have not been found to improve the rewarming process. Extubation criteria may differ among cardiothoracic groups, but at a minimum patients should be awake with stimulation and following commands, moving all extremities. Postoperatively, mediastinal bleeding, hemodynamic instability, respiratory failure, and stroke are the major risk factors for prolonged intubation. It is estimated that about 5% to 10% of patients are unable to be extubated early and remain intubated for 48 hours or longer. Mediastinal bleeding can either be "surgical"-meaning it requires repair and revision owing to a technical problem that can result from either arterial or venous bleeding-or it can be "medical" (which will not require surgical intervention). Even in the case of suspected surgical bleeding, control of coagulopathies, blood pressure (maintaining lowest perfusing pressures), and shivering can assist in decreasing bleeding, and its associated harm, until surgical intervention can be obtained. Causes of medical bleeding include preoperative and intraoperative anticoagulant medications, transfusion-associated coagulopathies, hypothermia, low calcium levels from transfusions, and underlying medical conditions predisposing the patient to coagulopathy, such as uremia, hepatic dysfunction, or underlying coagulopathies. Without active rewarming with forced air, hypothermia and its complications, particularly the prolongation of anesthetic time half-life, can also prolong intubation times. There is some evidence that the risk of wound infection also increases with 576 Pa rt 2 Critical Care Cardiovascular Disease they can be identified and treated in a more targeted manner. High chest tube output, while troubling, can be medically managed and temporized awaiting a surgical revision, if that is determined to be required. Immediate laboratory work should, along with clinical judgment and patient history, be used to identify any reversible coagulopathies to assist in temporizing or treating surgical or medical bleeding. A complication of cessation of bleeding using prothrombotic agents is clotting off the chest tubes and promoting cardiac tamponade.
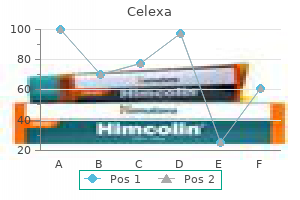
Cerebral blood flow autoregulation curves are depicted for normotensive (solid purple line) and chronic hypertensive (dashed blue line) states treatment hemorrhoids celexa 20 mg order on-line. The ideal medication to treat a hypertensive emergency should have a rapid onset of action, high potency, immediate reversibility, no tachyphylaxis, and minimal or no adverse effects. Although there is no perfect medication, several agents with some of these characteristics are summarized in Table 32. There are a limited number of studies comparing agents in terms of clinical outcomes. With no clear outcome data, the selection of an agent is based on the clinical scenario, pharmacologic characteristics of the drug, and availability. Parenteral agents that are useful in treating hypertensive emergencies are further discussed (in alphabetical order). Clevidipine has vasoselective properties with a rapid onset of action and a very short half-life (<1 minute). Clevidipine reduces blood pressure by a direct and selective effect on arterioles. It does not produce reflex tachycardia, and its effect on reducing afterload is often associated with increased cardiac output. The initial dose is usually 1 to 2 mg/h with adjustments as needed to obtain the desired response in blood pressure. The maintenance dose is usually 4 to 6 mg/h; however, higher doses may be required in certain clinical situations. Small studies have compared clevidipine to nitroprusside for the treatment of severe hypertension in anesthetized patients undergoing surgery. Although clevidipine has not been studied extensively in other clinical situations, its characteristics make it an attractive option for the treatment of hypertensive emergencies outside the operating room. In addition to its intraoperative use it has received increased attention in neurologic hypertensive emergencies. An alternative regimen is a continuous infusion starting at 1 to 2 mg/min and titrated upward to achieve a desired blood pressure endpoint. Adverse effects of labetalol include orthostatic hypotension, bronchospasm (should be avoided in asthma patients), heart failure, and significant bradycardia (should be avoided in the presence of sinus bradycardia or heart block greater than first degree). Labetalol has been shown to be effective in a wide range of clinical situations associated with hypertensive emergencies. However, because it does not affect renal function adversely and does not have increased toxicity in patients with renal failure, it may be a useful alternative to sodium nitroprusside in patients with hypertensive emergency and renal failure. Labetalol lowers blood pressure by decreasing systemic vascular resistance by 1-blockade and at the same time counteracts the reflex tachycardia from vasodilation through its -blocker effect. Nicardipine decreases systemic vascular resistance, without producing reflex tachycardia while maintaining or increasing cardiac output.
The analysis of the impact of a mild treatment xerostomia purchase celexa 40 mg visa, low-iodine, lotion soap on the reduction of nosocomial methicillinresistant Staphylococcus aureus: a new opportunity for surveillance by objectives. A crossover comparison of antiseptic soaps on nosocomial infection rates in intensive care units. Comparative efficacy of alternative handwashing agents in reducing nosocomial infections in intensive care units. Reduction in nosocomial transmission of drug-resistant bacteria after introduction of an alcoholbased handrub. Impact of alcohol-based, waterless hand antiseptic on the incidence of infection and colonization with methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci. Endemic aminoglycoside resistance in gram-negative bacilli: epidemiology and mechanisms. Are active microbiological surveillance and subsequent isolation needed to prevent the spread of methicillin-resistant Staphylococcus aureus Comparison of routine glove use and contact-isolation precautions to prevent transmission of multidrug-resistant bacteria in a long-term care facility. Prospective, controlled study of vinyl glove use to interrupt Clostridium difficile nosocomial transmission. Transmissibility of Clostridium difficile without contact isolation: results from a prospective observational study with 451 patients. Hospital-acquired infection with vancomycin-resistant Enterococcus faecium transmitted by electronic thermometers. Transmission of a highly drug-resistant strain (strain W1) of Mycobacterium tuberculosis. Efficacy of control measures in preventing nosocomial transmission of multidrug-resistant tuberculosis to patients and health care workers. Update: universal precautions for prevention of transmission of human immunodeficiency virus, hepatitis B virus, and other bloodborne pathogens in health-care settings. The contribution of a bacterially isolated environment to the prevention of infection in seriously burned patients. A comparison of the effect of universal use of gloves and gowns with that of glove use alone on acquisition of vancomycin-resistant enterococci in a medical intensive care unit. Effectiveness of gloves in the prevention of hand carriage of vancomycin-resistant Enterococcus species by health care workers after patient care.
Syndromes
Water ingestion can defend against the development of hypernatremia even when water losses are prodigious medications descriptions 40 mg celexa purchase free shipping. For that reason, hypernatremia upon presentation to the hospital occurs most commonly in patients who are incapacitated: those who have impaired thirst sensation, who cannot access water or who cannot express their need for water. Thus the development of hypernatremia in hospitalized patients is considered iatrogenic, reflecting an incomplete understanding of the factors that lead to hypernatremia. To counteract cellular volume contraction, cells begin to adapt within minutes by allowing the influx of electrolytes, thus mitigating cell shrinkage. When hypernatremia lasts more than a few hours, brain cells generate new organic osmolytes. This leads to further water movement back into brain cells, restoring cell volume to near normal after about 3 days. Most often, patients with long-standing hypernatremia present with weakness, lethargy, and confusion. Acute severe hypernatremia in infants and small children is associated with intracranial bleeding,228 presumably caused by brain shrinkage and traction on the penetrating vessels. There is some controversy, however, as to whether the hypernatremia in that situation is the cause or the effect of the intracranial hemorrhage. Hypernatremic patients who appear euvolemic most likely have pure water loss as an explanation for their hypernatremia. This is because the water is lost from all body compartments proportionately; only one-twelfth of the water loss is intravascular. For example, a 60-kg woman with a 3-L pure water loss would experience an intravascular loss of only 250 mL (clinically imperceptible) but would develop a plasma sodium concentration of 155 mmol/L. Pure water can be lost either through the skin and respiratory tract (so-called insensible losses) or in urine. Insensible losses amount to about 10 mL/kg body weight per day under normal environmental conditions in an afebrile individual with a normal respiratory rate. Thus hypernatremia (plasma sodium *Hyponatric and hypernatric are used here to refer to a fluid with a sodium concentration less than (or greater than) that of plasma. Of special interest to intensivists is a classic triphasic syndrome that may be seen following severe head trauma: 1. Initially, there is abrupt cessation of vasopressin release from the posterior pituitary, accompanied by polyuria. About a week later, an antidiuretic phase ensues, characterized by urinary concentration and water retention with a tendency toward hyponatremia, lasting 5 to 6 days. This appears to result from the release of stored vasopressin from the degenerating hypothalamic neurons. They develop hypernatremia only with water deprivation, owing to mental or physical incapacity, and/or neglect. For example, if the 60-kg woman whose plasma sodium concentration rose to 155 mmol/L (see earlier) had lost the equivalent of half-isotonic saline solution instead of pure water, her intravascular volume would have contracted by 750 mL, enough to cause at least orthostatic hypotension and tachycardia.
Peripartum cardiomyopathy symptoms quitting weed generic 40 mg celexa with mastercard, transient apical ballooning syndrome ("takotsubo" or stress cardiomyopathy), cardiomyopathy associated with prolonged tachycardia, and cardiomyopathy related to cardiotoxic cancer chemotherapy are less common. Uncommon causes are alcoholic cardiomyopathy, diabetic cardiomyopathy, and a cardiomyopathy seen in some patients with hyperthyroidism or severe obesity. Sympathetic nervous system activation results in tachycardia, arrhythmias, increased myocardial oxygen consumption, and peripheral vasoconstriction. Weakened left ventricular contractile force and neurohormonal activation lead to changes in cardiac structure termed ventricular remodeling. A detrimental positive feedback loop is established, where further left ventricular dysfunction leads to intensification of maladaptive responses, progressive deterioration in left ventricular structure and performance, and worsening heart failure. Uncommon conditions leading to diastolic heart failure include infiltrative and restrictive cardiomyopathies, such as amyloid cardiomyopathy, and chronic constrictive pericarditis. A report on the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for Evaluation and Management of Heart Failure): Developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: Endorsed by the Heart Rhythm Society. Symptoms of heart failure caused by pulmonary or systemic venous congestion are shortness of breath with exertion or at rest, cough, swelling of legs and/or abdomen, orthopnea, and paroxysmal nocturnal dyspnea. Fatigue, anorexia, and change in mental status are symptoms caused by low cardiac output. Physical examination findings include pulmonary rales, elevated jugular venous pressure, signs of cardiomegaly, cardiac murmurs (especially mitral regurgitation), S3 gallop, hepatic enlargement, ascites, and edema. An S3 gallop and elevated jugular venous pressure are the most specific signs of heart failure; absence of rales is not infrequent in patients with acute heart failure, and chest radiography may not show obvious congestion. A careful evaluation for the presence of pulsus paradoxus is important if cardiac tamponade is suspected. However, these signs and symptoms are not specific for heart failure, and coexisting conditions, such as obesity, chronic lung disease, and deconditioning, can add uncertainty to the clinical diagnosis. Heart failure is often both underdiagnosed and overdiagnosed in outpatient and emergency department settings. Levels between 100 and 400 pg/mL can be seen in patients with primary right ventricular failure owing to cor pulmonale with chronic lung disease, idiopathic pulmonary hypertension, and acute pulmonary embolism. Total hospital stay was shortened by 3 days, cost of treatment was significantly reduced, and time to initiation of definitive therapy in the emergency department was shortened by 30 minutes. Higher levels are seen in patients with more severe heart failure and with worse left ventricular systolic function. Higher levels are correlated with a poorer prognosis and can predict an increased rate of functional deterioration and mortality. Competing risk of cardiac status and renal function during hospitalization for acute decompensated heart failure. It is cleared from the serum by the kidneys, so levels are higher in patients with coexisting renal disease. Most recent data from the United States in the Medicare population show a 1-year mortality of 29.
Patients whose conditions have not improved after 14 to 21 days of therapy with specific chemotherapy plus corticosteroids have an exceedingly poor prognosis withdrawal symptoms cheap celexa 20 mg mastercard. Corticosteroids should not generally be used to treat elevated intracranial pressure in this situation. Lesions are characteristically enhancing in a ringlike pattern and typically occur in the basal ganglia, but many different radiologic presentations have been documented. However, some laboratories use less sensitive assays and thus some patients may appear to be seronegative. Most patients who have toxoplasmosis will show clinical and radiologic improvement within 2 weeks. If such improvement has not been documented, and the diagnosis is in doubt, a needle biopsy of the intracranial lesion should be considered. Therapy for lymphoma should be determined in consultation with experienced oncologists. The therapy of choice for cryptococcal meningitis in the United States is liposomal amphotericin B for at least 2 weeks, plus oral flucytosine. Fluconazole should not be used for initial therapy, although it can be used after the initial 2 weeks if patients have a good clinical response. If results of stool cultures are negative, testing samples for ova and parasites might be indicated if there is a history compatible with exposure. Isoniazid prophylaxis is important for any patient with a tuberculin skin test that shows more than 5 mm of induration or a history of substantial recent exposure. Thus evaluating hypotension in this patient population requires a comprehensive and thorough approach. Prevention of Opportunistic Infection Intensivists usually focus on the management of acute processes, but if attention is not provided to opportunistic infection prevention, patients hospitalized for one process may develop a second lifethreatening process given the high incidence of opportunistic infections. Primary prophylaxis is the term used to indicate strategies that reduce the likelihood of an initial episode of a disease process. Secondary prophylaxis is the term that was used to indicate strategies that prevent reinfections and recurrences; chronic maintenance is the term used for strategies to prevent relapses. More recently, such prophylaxis is referred to as chronic suppression if the goal is to prevent a relapse, and secondary prophylaxis if the goal is to prevent reinfection. It is clear that initiating therapy within a period of hours rather than days is best. Many authorities now advocate an antiretroviral regimen for any situation when the patient and health care provider determine that therapy is appropriate and continuation of that therapy for 4 to 6 weeks. Organ transplant recipients develop a different spectrum of infections than patients with cancer-related neutropenia. Donor-derived transmission events in 2013: a report of the Organ Procurement Transplant Network Ad Hoc Disease Transmission Advisory Committee. Innate immunity in plants: an arms race between pattern recognition receptors in plants and effectors in microbial pathogens. Quantitative relationships between circulating leukocytes and infection in patients with acute leukemia.
Which of the following statements is most correct regarding use of antihypertensive agents for the therapy of a hypertensive crisis Nitroprusside alone is the therapeutic agent of choice for lowering the blood pressure in an acute aortic dissection 5 medications for hypertension 10 mg celexa order. With a short-acting intravenous drug, the clinician has the ultimate control on achieving a precise blood pressure target. Oral therapy can be used to treat some hypertensive urgencies such as postoperative hypertension with a functioning gut. Reduction of the blood pressure to less than 90 mm Hg systolic, or even by as little as 35% of the initial mean arterial pressure, has been associated with major organ dysfunction, coma, and death. In hypertensive crises the mean blood pressure should be initially reduced by 15% to 20%. Nitroprusside, when used to treat hypertension associated with a dissecting aortic aneurysm, should be used in combination with an intravenous -blocker. Which of the following factors is most important in determining the need to immediately decrease the blood pressure in a patient presenting with an ischemic stroke Management of hypertension in the setting of an acute ischemic stroke is based on an understanding of changes that occur in the capacity to autoregulate blood flow in the injured brain. Decreases in blood pressure can cause secondary neurologic injury be expanding the infarct size. Based on this concept, current recommendations are to tolerate high blood pressures in the setting of an acute ischemic stroke. The main factor to change this approach would be the use of systemic thrombolytics. In patients receiving thrombolytics the systolic blood pressure must be keep below 180 mm Hg to decrease the risk of hemorrhage. Which of the following is most correct concerning treatment of hypertension associated with aortic dissection Blood pressure target with aortic dissection is a 25% reduction in mean arterial pressure. Blood pressure lowering target with aortic dissection should be achieved within first hour. Avoiding dropping blood pressure below the autoregulatory range is paramount in the therapy of aortic dissection. Rationale: Reducing the shearing force characterizes the rate of change of pressure with respect to time (or dP/dt, the aortic pulse wave [first derivative of pressure measured over time]) to minimize the impact of each cardiac cycle on dissection and is one of the most important principles of therapy of elevated blood pressure with aortic dissection.
Which of the following is least likely to precipitate ventilatory failure in a patient with myasthenia gravis There is a long list of medications that can exacerbate weakness in patients with myasthenia gravis 300 medications for nclex purchase 40 mg celexa amex. Chief among these calcium channel blockers, -blockers, antiarrhythmic agents, and antibiotics such as aminoglycosides, macrolides, and fluoroquinolones. Others include antimalarials, corticosteroids, and anticonvulsants such as carbamazepine, gabapentin, and phenytoin. A 70-kg 65-year-old man who is 5 foot 9 inches tall is diagnosed with myasthenia gravis and has been receiving increasing doses of pyridostigmine. He is able to move all extremities but has mild fatigability to repetitive testing of his deltoids. Handheld spirometry shows a negative inspiratory force of -50 cm H2O and vital capacity of 1. This patient is exhibiting signs of a myasthenic crisis and the most immediate treatment for improvement would be to administer an acetylcholinesterase inhibitor. He does not have signs of overtreatment with a cholinergic crisis, which would include bradycardia, diarrhea, and bronchorrhea, and there are few risks to administering more pyridostigmine. Endotracheal intubation should always be considered in a patient in myasthenic crisis; however, if the patient is not in respiratory distress, handheld spirometry can help determine the need for intubation. A negative inspiratory force of less than 20 cm/ H2O or vital capacity of less than 20 mL/kg would be indicators for immediate intubation. Therapy with pyridostigmine may help avert the need for intubation; however, the patient will need to be continuously monitored for signs of worsening. As to the former, whenas the fits are often repeated, and every time grow more cruell, the animal functions are quickly debilitated; and from thence, by the taint, by degrees brought on by the Spirits, and the Nerves serving the Praecordia, the vital function is by little and little enervated, till at length, the whole body languishing, and the pulse is loosned, and at length ceasing, at last the vital flame is extinguished. And most importantly, several interventions required for treatment of refractory seizures, such as mechanical ventilation and vasopressor usage, require the expertise of an intensivist in addition to a neurologist. Other risk factors include chronic or acute renal failure, administration of medications that may lower seizure threshold (such as penicillins, carbapenems, cefepime,22 meperidine, cyclosporine, and neuroleptics) and any rapid osmolar shifts such as those induced during treatment of sodium abnormalities or hemodialysis. Hyperglycemic crises, either nonketotic or ketotic, have a high likelihood of focal seizures,23,24 and treatment of these should focus on correcting the electrolyte abnormality. Nosology and Semiology Numerous systems have evolved for the classification of seizures; the most frequently used today is that of the International League Against Epilepsy26 (Box 62.
Mazin, 43 years: Initially 5 to 10 minutes in duration, T-tube trials are extended and repeated several times a day until the patient can sustain spontaneous ventilation for several hours. Mineralocorticoid excess may be the cause if the renal potassium loss is associated with systemic hypertension, and the reninaldosterone axis should be studied with basal and saline solution� suppressed blood hormone measurements. Several strategies to provide enteral feeding without increasing gastric colonization with pathogenic microorganisms have been tried. After elective cardioversion anticoagulation is indicated for 4 to 6 weeks because there is a lag between the mechanical function and electrical restoration of sinus rhythm that may allow for thrombus formation.
Emet, 51 years: Emergency endovascular stent-grafting for life-threatening acute type B aortic dissections (Commentary). In fact, there was more pneumonia and septic shock in the placebo group than in the steroid-treated group. Treatment of refractory status epilepticus with propofol: clinical and pharmacokinetic findings. Experts have recently suggested that measurement of free cortisol levels makes more physiologic sense, but studies have not helped establish diagnostic thresholds for free cortisol levels.
References