



Anamarija Morovic?, MD
Asendin dosages: 50 mg
Asendin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 360 pills

Maxillary Nerve Block the maxillary nerve exits the skull through the foramen rotundum and gives its terminal branches depression endogenous symptoms order asendin 50 mg without a prescription. Except for the middle meningeal nerve, innervating the dura mater, all branches (zygomatic branches, superior alveolar nerve, pterygopalatine and parasympathetic branches, palatine and pharyngeal branches) arise in the pterygopalatine fossa to the face. At the upper part of the pterygopalatine fossa, the maxillary nerve is accessible for a complete maxillary block. The nerve territory blocks are the lower eyelid, ala of the nose, cheek, upper lip, cutaneous zygomatic and temporal zone on the face and superior teeth, palatine zone, maxillary bone. The suprazygomatic approach to the maxillary nerve in pterygopalatine fossa seems to be the safest and is easily reproducible in children. The needle (22 to 25 gauge) is inserted perpendicular to the skin and advanced to reach the greater wing of the sphenoid at a depth of approximately 10 to 15 mm. The needle is then reoriented in a caudal and posterior Posterior orbital rim Puncture point direction and advanced 35 to 45 mm deep to the pterygopalatine fossa. Ultrasound guidance technique is possible with the ultrasound transducer located in the infrazygomatic area, over the maxilla, with an inclination of 45 degrees in both the frontal and horizontal planes. The probe location allows visualization of the pterygopalatine fossa, limited anteriorly by the maxilla and posteriorly by the greater wing of the sphenoid. This real-time ultrasound-guided technique is easy and ensures the correct location of local anesthetic injection in the pterygopalatine fossa. The mandibular nerve, the largest branch of the trigeminal nerve, exits from the cranium through the foramen ovale of the greater wing of the sphenoid. The anterior trunk is formed with branches serving mainly motor innervation to temporalis, masseter, pterygoids, mylohyoid, and tensor tympani and palati muscles and the buccal nerve. Auriculotemporal, lingual, and inferior alveolar nerves comprise the posterior trunk. The needle was inserted perpendicular to the skin (A) and advanced to reach the greater wing of the sphenoid at approximately 10 to 15 mm depth (B). Reorientation of needle in a caudal and posterior direction (C) and advancement of 35 to 45 mm deep to the pterygopalatine fossa (D and E). The puncture area is bounded by the zygomatic arch at the top and the mandibular notch just anterior to and below the tragus of the ear. The needle entry point is located in the sigmoid fossa between the coronoid and condylar process of the ramus of the mandible. To avoid the risk for arterial puncture, it is recommended to prick as high as possible in the space between the zygomatic arch and the center of mandibular notch.
Diseases
Fluid balance is a fundamental aspect to control in the patient who is critically ill with anuria depression symptoms on dogs purchase 50 mg asendin free shipping. All patients who are critically ill need a high daily amount of volume infusions-blood and fresh frozen plasma, vasopressors and other continuous infusions, and parenteral and enteral nutrition, which should be delivered without restriction or interruption. The consequent positive fluid balance and tendency to interstitial edema cause the necessity for water removal and, possibly, the achievement of a negative daily fluid balance. In particular, when volemic and uremic control is not a problem, an aggressive, protein-rich nutritional policy (1. This phenomenon is driven by hydrostatic and osmotic forces and allows for the elimination of high plasma water volumes each day with a reduced risk of hypovolemia and hypotension. In children who are critically ill, the correction of water overload is considered a priority; it has been shown and recently confirmed that restoring adequate water content in small children is the main independent variable for outcome prediction. This marker solute should be reasonably representative of all solutes that are normally removed from blood by the kidney. Furthermore, despite its moderate toxicity, urea is the final product of protein metabolism; its accumulation describes the need for dialysis and its removal describes treatment efficiency. It is a small molecule, and its volume of distribution is similar to total body water. It is not bound to protein, and it freely passes through tissues and cell membranes. Creatinine has similar characteristics and is another commonly used marker solute. The intensity of a dialytic treatment can be roughly indicated by the amount of dialysis and hemofiltration flow delivered to the patient. As a consequence, the definition of normal dose is now recommended in a range of 20 to 30 mL/kg/hr for continuous therapies or three times per week intermittent hemodialysis, or both. Downtime attributable to filter-circuitcatheter clotting, circuit change, frequent replacement solution-bag substitution, and patient mobility (surgery, diagnostics) should be carefully monitored and might significantly affect the dialysis dose. The level of attention is probably greater when a dedicated dialysis nurse administers the therapy for few hours during the day shift. The predictive ability of urine output was negatively affected by the use of diuretic agents. It is possible, on the other hand, that patients with signs of only partial renal recovery may benefit from more specific and prolonged weaning algorithms. This is done to increase the pressure inside the membrane lung by adding the downstream resistance exerted by the hemofilter. Furthermore, the need for heparin is minimized by diluting the blood entering the membrane lung with the plasma water separated by the hemofilter.
Fanard L anxiety urination cheap asendin 50mg visa, Van Steenberge A, Demeire X, et al: Comparison between propofol and midazolam as sedative agents for surgery under regional anaesthesia, Anaesthesia 43(Suppl):87-89, 1988. Royal College of Anaesthetists and British Society of Gastroenterology joint working party. Berkenstadt H, Perel A, Hadani M, et al: Monitored anesthesia care using remifentanil and propofol for awake craniotomy, J Neurosurg Anesth 13(3):246-249, 2001. Ryu J-H, Kim J-H, Park K-S, et al: Remifentanil-propofol versus fentanyl-propofol for monitored anesthesia care during hysteroscopy, J Clin Anesth 20(5):328-332, 2008. Casati A, Fanelli G, Casaletti E, et al: Clinical assessment of targetcontrolled infusion of propofol during monitored anesthesia care, Can J Anaesth 46:235-239, 1999. Sakaguchi M, Higuchi H, Maeda S, et al: Dental sedation for patients with intellectual disability: a prospective study of manual control versus Bispectral Index-guided target-controlled infusion of propofol, J Clin Anesth 23(8):636-642, 2011. Ahmad S, Yilmaz M, Marcus R-J, et al: Impact of bispectral index monitoring on fast tracking of gynecologic patients undergoing laparoscopic surgery, Anesthesiology 98:849-852, 2003. Millar J: Fast-tracking in day surgery: is your journey to the recovery room really necessary McCleane G: Novel approaches to postoperative analgesia for day case surgery: a review, J One-day Surg 18(1):4-8, 2008. Michaloliakou C, Chung F, Sharma S: Preoperative multimodal analgesia facilitates recovery after ambulatory laparoscopic cholecystectomy, Anesth Analg 82(1):44-51, 1996. Eriksson H, Tenhunen A, Korttila K: Balanced analgesia improves recovery and outcome after outpatient tubal ligation, Acta Anaesthesiol Scand 40(2):151-155, 1996. Hartmann T, Hoerauf K, Zavrski A, et al: Light to moderate sedation with sevoflurane during spinal anesthesia, Acta Anaesthesiol Scand 42(Suppl 112):221-222, 1998. Pavlovic D, Usichenko T: B-Aware: recall of intraoperative events (letter), Lancet 364(9437):841, 2004. In Gullo A, editor: Anaesthesia, pain, intensive care and emergency medicine, Milano, 1996, SpringerVerlag, pp 1003-1011. Chauvin M: State of the art of pain treatment following ambulatory surgery, Eur J Anaesthesiol 20(Suppl 28):3-6, 2003. Rawal N, Allvin R, Amilon A, et al: Postoperative analgesia at home after ambulatory hand surgery: a controlled comparison of tramadol, metamizol, and paracetamol, Anesth Analg 92(2):347-351, 2001. Etropolski M, Kelly K, Okamoto A, et al: Comparable efficacy and superior gastrointestinal tolerability (nausea, vomiting, constipation) of tapentadol compared with oxycodone hydrochloride, Adv Ther 28(5):401-417, 2011. Capdevila X, Macaire P, Aknin P, et al: Patient-controlled perineural analgesia after ambulatory orthopedic surgery: a comparison of electronic versus elastomeric pumps, Anesth Analg 96(2):414-417, 2003. Wallenborn J, Gelbrich G, Bulst D, et al: Prevention of postoperative nausea and vomiting by metoclopramide combined with dexamethasone: randomised double blind multicentre trial, Br Med J 333(7563):324, 2006.
When the staining appears too pink or red great depression definition economics generic asendin 50 mg line, the usual problem is buffer that is too acidic. Other causes of excessive red or pink coloration include inadequate staining times or excessive washing of the slide. Most often, problems with staining are caused by problems with the pH of the solutions, and use of new buffer solutions often corrects the problem. The number of leukocytes may be estimated by scanning the blood film at an intermediate power. Mechanical effects leading to abnormal distribution of larger cells should be excluded by examination of the edges of the blood film in particular. Care must be taken when making the smear because cells, particularly neoplastic cells, may be more easily disrupted by excessive mechanical pressure than normal leukocytes. Significant artifacts begin to be observed in blood that has been held for several hours and include cytoplasmic vacuolation, nuclear karyorrhexis, and cytoplasmic disruption. The presence of immature myeloid cells (myelocytes, metamyelocytes, promyelocytes, and blasts) is distinctly abnormal. For example, infection or growth factor therapy often leads to increased prominence of the primary (azurophilic) granules in neutrophils, termed toxic granulation. Bone marrow examination usually involves two separate, but interrelated, specimens. The first is a cytologic preparation of bone marrow cells obtained by aspiration of the marrow and a smear of the cells, allowing excellent visualization of cell morphology and enumeration of the marrow cellular elements. Before a bone marrow examination is performed, clear diagnostic goals about the information to be obtained from the procedure should be defined and decisions made about whether any special studies are needed, to ensure that all necessary specimens may be collected and handled correctly. However, by early childhood, fat cells begin to replace the bone marrow hematopoietic cells in the extremities so that adults have hematopoiesis limited to the axial skeleton and proximal portions of the extremities. Sternal marrows do not allow a biopsy to be performed, and several possible complications, including hemorrhage and pericardial tamponade, may occur if the inner table of the sternum is penetrated by the needle at areas other than the second intercostal space. The sternal marrow space in an adult is only approximately 1 cm thick at the second intercostal space, so care must be taken to avoid penetrating the chest cavity, although sternal bone marrow needles have guards to prevent penetration of the needle beyond the sternal plate. In contrast, little morbidity is associated with iliac crest aspiration and biopsy, and the posterior iliac crest is the most common site for bone marrow sampling. Wet preparations are made by placing a drop of blood on a slide, covering the drop with a coverslip, and surrounding the coverslip with petroleum jelly or paraffin wax to seal the edges. If needed, the blood may be diluted with isotonic saline, or in some cases, it may be fixed with buffered glutaraldehyde for later examination. Some organisms, such as spirochetes and trypanosomes, may be detected by movement in wet mount preparations although more definitive testing, such as serology or molecular organism detection is more frequently used.
Croton eluteria (Cascarilla). Asendin.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96217
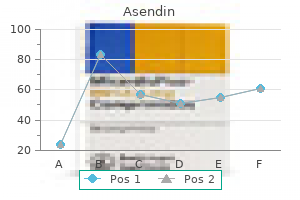
Units vary across agents for single dose (mg versus g) and continuous infusion (mg/hr versus g/hr) symptoms depression versus bipolar asendin 50mg purchase free shipping. Mean and standard deviation of visual analogue pain scores (y axis) for both epidural analgesia (represented by dark blue circles) and parenteral opioids (represented by open red circles) for each postoperative day (x axis) up to the fourth day after surgery. The analgesic site of action (spinal versus systemic) of continuous epidural infusion of lipophilic opioids is not clear. Although some data suggest a benefit from epidural (versus intravenous) infusion of lipophilic opioids,82 the overall advantage of administering continuous epidural infusion of lipophilic opioids alone is marginal. Continuous infusion of a hydrophilic opioid may be especially useful for providing postoperative analgesia when the site of catheter insertion is not congruent with the site of surgery or when side effects. Use of a continuous infusion rather than intermittent boluses of epidural morphine may result in superior analgesia with fewer side effects. Use of a local anesthetic and an opioid in an epidural infusion may have advantages over infusions consisting of a local anesthetic or opioid alone. In general, bupivacaine, ropivacaine, or levobupivacaine is chosen because of the differential and preferential clinical sensory blockade with minimal impairment of motor function. Concentrations used for postoperative epidural analgesia are lower than those used for intraoperative anesthesia. The choice of opioid also varies, although many clinicians prefer a lipophilic opioid. A variety of adjuvants may be added to epidural infusions to enhance analgesia while minimizing side effects, but none has gained widespread acceptance. Clonidine mediates its analgesic effects primarily through the spinal dorsal horn 2-receptors on primary afferents and interneurons, as well as the descending noradrenergic pathway, and the epidural dose typically used ranges from 5 to 20 g/hr. Epinephrine may improve epidural analgesia, can increase sensory blockade, and is generally administered at a concentration of 2 to 5 g/ mL. Location of Catheter Insertion Insertion of the epidural catheter congruent to the incisional dermatome. Furthermore, the benefits of epidural analgesia in decreasing morbidity in patients undergoing abdominal and thoracic surgery are seen only with thoracic (congruent), not lumbar (incongruent), epidural catheter placement. Standing orders and nursing protocols for analgesic regimens, neurologic monitoring, treatment of side effects, and physician notification about critical variables should be standard for all patients receiving neuraxial and other types of postoperative analgesia (see Box 98-1). The local anesthetics used in an epidural analgesic regimen may block sympathetic fibers and contribute to postoperative hypotension.
The optimal time for initiating targeted Sudden Unexplained Deaths Unexpected and unexplained deaths in infants to young adults may be associated with genetic variations or mutations of ion channels in myocardial cells depression music asendin 50mg generic. Channelopathies allow abnormal electrolyte movement across myocardial cell membranes, predisposing the heart to irregular depolarizations and arrhythmias. Interfacility transfer should be considered if a survivor of cardiac arrest arrives at a hospital that does not have the capability of providing targeted temperature management since hours between resuscitation and the initiation of the therapy has been demonstrated to provide benefit. American Heart Association in collaboration with International Liaison Committee on Resuscitation: Circulation 102(Suppl):I1I370, 2000. Although the best treatment algorithm for survivors of cardiac arrest is currently unknown, coordinated, consistent care provided by experienced health care professionals in a facility with multiple advanced interventions available and a review process for the care rendered to survivors of cardiac arrest all contribute to optimized care and will likely contribute to improved patient outcomes. Working with such extraordinary talent is certainly a professional highlight in my career. Emergency Cardiac Care Committee and Subcommittees: American Heart Association: proceedings of the 1992 National Conference on Cardiopulmonary Resuscitation and Emergency Cardiac Care, Ann Emerg Med 22:275-511, 1993. American Heart Association in collaboration with International Liaison Committee on Resuscitation: Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care: a Consensus on Science, Parts 1-12, Circulation 102:I1-I370, 2000. Harada Y, Fuseno H, Ohtomo T, et al: Self-administered hyperventilation cardiopulmonary resuscitation for 100 s of cardiac arrest during Holter monitoring, Chest 99:1310-1312, 1991. Tibballs J, Russell P: Reliability of pulse palpation by healthcare personnel to diagnose pediatric cardiac arrest, Resuscitation 80: 61-64, 2009. Steen S, Liao Q, Pierre L, et al: the critical importance of minimal delay between chest compressions and subsequent defibrillation: a haemodynamic explanation, Resuscitation 58:249-258, 2003. Christenson J, Andrusiek D, Everson-Stewart S, et al: Chest compression fraction determines survival in patients with out-of-hospital ventricular fibrillation, Circulation 120:1241-1247, 2009. Callaham M, Barton C: Prediction of outcome of cardiopulmonary resuscitation from end-tidal carbon dioxide concentration, Crit Care Med 18:358-362, 1990. Kalenda Z: the capnogram as a guide to the efficacy of cardiac massage, Resuscitation 6:259-263, 1978. Dorian P, Cass D, Schwartz B, et al: Amiodarone as compared with lidocaine for shock-resistant ventricular fibrillation, N Engl J Med 346:884-890, 2002. Lin T, Chen Y, Wang M: Use of transesophageal echocardiography during cardiac arrest in patients undergoing elective noncardiac surgery, Br J Anaesth 96:167-170, 2006. Price S, Uddin S, Quinn T: Echocardiography in cardiac arrest, Curr Opin Crit Care 16:211-215, 2010. Salen P, Melniker L, Chooljian C, et al: Does the presence or absence of sonographically identified cardiac activity predict resuscitation outcomes of cardiac arrest patients Laver S, Farrow C, Turner D, et al: Mode of death after admission to an intensive care unit following cardiac arrest, Intensive Care Med 30:2126-2128, 2004. Hypothermia after Cardiac Arrest Study Group: Mild hypothermia to improve the neurologic outcome after cardiac arrest, N Engl J Med 346:549-556, 2002. Nielsen N, Sunde K, Hovdenes J, et al: Adverse events and their relation to mortality in out-of-hospital cardiac arrest patients treated with therapeutic hypothermia, Crit Care Med 39:57-64, 2011.
Other factors to be considered are the presence of pulmonary hypertension depression symptoms teenage males asendin 50 mg buy low price, electrical rhythm disorders, and other comorbidities. It is usually desirable to return the patient to an arousable, sedated state with spontaneous ventilation at the end of the procedure in the presence of normal homeostasis and absence of complications. The causes may be an inadequate surgical result with a residual defect requiring repair, pulmonary artery hypertension, or right or left ventricular dysfunction. This is due to several factors: (1) A disproportionate exposure to the nonendothelialized extracorporeal circuit produces an inflammatory-like response. The immediate postoperative period, even that of normal convalescence, is one of continuous physiologic change because of the pharmacologic effects of residual anesthetic agents and the ongoing physiologic changes secondary to abrupt alteration in hemodynamic loading conditions, surgical trauma, and extracorporeal circulation. Cardiac surgery is an established and effective treatment for children with congenital heart defects. In turn, these accomplishments gave rise to the development of pediatric cardiac anesthesiologists, individuals who understand the pathophysiology of congenital heart malformations, the diagnostic and surgical procedures used to treat heart disease, and the principles of pediatric and cardiac anesthesia and intensive care medicine. Pediatric cardiac anesthesia continues to evolve as an exciting and technically demanding subspecialty in which anesthetic management is based on physiologic principles. Management of patients under these physiologic extremes is a vital function of the pediatric cardiovascular anesthesiologist. We assume that the reader already understands the fundamentals of adult cardiac (see Chapter 67) and general pediatric anesthesia (see Chapter 93). Under such circumstances, the continued presence of a transitional circulation can lead to severe hypoxemia, acidosis, and hemodynamic instability, which are poorly tolerated in the neonate. Importantly, the transitional circulation can be manipulated by pharmacologic ventilatory strategies, thereby promoting hemodynamic stability in the pediatric patient. Another unique feature of the normal neonatal and infant cardiovascular system is the reduced myocardial reserve in contrast to that in the healthy adult. Although the resting performance of the neonatal myocardium may be greater than in adults and older children, sensitivity to -blockade is greater and only modest increases occur in cardiac performance after administration of the -agonist drugs dobutamine and isoproterenol. Large nuclei, mitochondria, and surface membranes predominate within the myofibrils. In neonates, a 50% reduction in the number of myofibrils is seen and the myofibrils are arranged in a nonlinear, disordered array. However, when left-sided filling pressures exceed 7 to 10 mm Hg, further increases in left ventricular stroke volume are minimal. The transverse tubular system is absent, and the sarcoplasmic reticulum, which has to store and release calcium, is small and inefficient. The neonatal heart therefore depends more on extracellular calcium levels than the adult myocardium. This is in contrast to adult cardiac patients in whom calcium use during cardiac surgery has fallen into some disfavor, owing to direct concerns over myocardial ischemia and reperfusion injury. The pulmonary circulation undergoes significant changes during the first months of life.
As an initial screening tactic depression symptoms hallucinations 50 mg asendin purchase with mastercard, articles are vetted by the working group or "task force" of 8 to 12 individuals from relevant diverse backgrounds. A comprehensive literature search attempts to capture all relevant articles identified through both electronic and manual searches. The search is systematic to the extent that it is guided by the defined boundaries of the search protocol and the expected outcomes associated with the identified clinical interventions. Use of a methodology that properly incorporates a comprehensive and systematic literature search protocol can reduce potential biases that may not otherwise be recognized during a less rigorous search. Organizing and summarizing data from a large number of articles are facilitated by using a "data extraction" spreadsheet or table in which patient outcome data associated with each intervention are recorded and categorized (Tables 112-1 to 112-3). This tabular method of organizing outcome data, arranged by intervention, allows for the recording of critical analytic features. This tabulation facilitates the narrative reporting of findings, as well as the recording of data that can subsequently be used for formal statistical analyses. Moreover, the presentation of outcomes in this format is useful for detecting whether different patterns of outcomes are associated with an intervention and can also highlight the occurrence of rare or unique outcomes. In addition to a detailed recording of the clinical outcomes reported in each reviewed study, studies are also evaluated on the basis of research design, sample size, scale of measurement, power, and other traditional statistical parameters. The outcome findings reported in these studies are aggregated only if the patients in the different studies received essentially the same type of treatment and if similar types of patients. Each of these safeguards is predicated on an underlying concern with the identification and management of bias. Identifying and managing bias are critical to the effective collection and synthesis of evidence. Practical countermeasures instituted for each type of bias are described in the following subsections. Selected data from American Society of Anesthesiologists: Practice guidelines for central venous catheterization, Anesthesiology 116:539-573, 2012. Detailed information can be found in the data extraction workbook of the Guidelines. This diversity helps ensure that the set of articles selected by the task force is as comprehensive as possible. Article selection bias can also arise when editorials, letters, and position papers are used as sources of scientific evidence. These types of articles are often written to promote a particular point of view regarding an intervention or outcome of concern. Although some editorials and letters are informative and well documented, they likely have not been subjected to the same level of peer review as original research papers. The authors of these articles may or may not be experts, may rely on a narrowly selected subset of the literature, or may have intentionally written the article to be "controversial. Such a reviewer may not be fully cognizant of the constraints of the data or the proper context for analyzing and interpreting the reported findings.

Effect of hypobaricity on hypoxic ventilatory response in humans depression transfer buy discount asendin 50 mg line, Anesthesiology 85(Suppl):A1121, 1996. Bendz B, Rostrup M, Sevre K, et al: Association between acute hypobaric hypoxia and activation of coagulation in human beings, Lancet 356:1657-1658, 2000. Air travel in patients with chronic obstructive pulmonary disease, Arch Intern Med 151: 1793-1795, 1991. Evaluation of patients with chronic airway obstruction, Am Rev Respir Dis 130:980-986, 1984. Aerospace Medical Association Air Transport Medicine Committee: Medical guidelines for air travel, Aviat Space Environ Med 67:B1-16, 1996. Nyhan D, Kim S, Dunbar S, et al: Impaired pulmonary artery contractile responses in a rat model of microgravity: role of nitric oxide, J Appl Physiol 92:33-40, 2002. Mechanism of spaceflight-induced changes in left ventricular mass, Am J Cardiol 95:1128-1130, 2005. Beck G: Emergency airway management in orbit: an evidence-based review of possibilities, vii Respir Care Clin N Am 10:401-421, 2004. Potential anesthesia protocols for space exploration missions, Aviat Space Environ Med 84:226-233, 2013. Marescaux J, Leroy J, Gagner M, et al: Transatlantic robot-assisted telesurgery, Nature 413:379-380, 2001. Haidegger T, Sandor J, Benyo Z, et al: Surgery in space: the future of robotic telesurgery, Surg Endosc 25:681-690, 2011. Safar P, Tenicela R: High altitude physiology in relation to anesthesia and inhalation therapy, Anesthesiology 25:515-529, 1964. Bandholz Frank L: General anesthesia at high altitudes, J Am Med Womens Assoc 13:317-319, 1958. Pederson L, Benumof J: Incidence and magnitude of hypoxaemia with ketamine in a rural African hospital, Anaesthesia 48:67-69, 1993. Propofol-fentanyl anaesthesia at high altitude: anaesthetic requirements and haemodynamic variations when compared with anaesthesia at low altitude, Acta Anaesthesiol Scand 52:427-431, 2008. Aeromedical evacuation of patients with pneumocephalus: outcomes in 21 cases, Aviat Space Environ Med 79:30-35, 2008. Commercial air travel and in-flight pulmonary hypertension, Aviat Space Environ Med 84:65-67, 2013.
Arakos, 31 years: Many interventional specialists are consultants, not involved in the primary care of the patients they are treating.
Raid, 46 years: Mohr H: the design of x ray equipment for use in operating rooms, Med Biol Eng 11:396-403, 1973.
Abe, 41 years: The system is unable to keep up with an ever-expanding proliferation of new services, new sites, and new practitioners.
References