




Rajan A.G. Patel, MD
Pirfenex dosages: 200 mg
Pirfenex packs: 90 pills, 180 pills, 270 pills, 360 pills
B symptoms 10 days before period purchase 200 mg pirfenex with amex, Prostatic acini consist of a double layer of epithelial cells (E), which line the lumen, and basal cells (B), which give rise to epithelial cells. Acknowledgements Robert P Myers, Emeritus Professor of Urology, and Akira Kawashima and Bernard F King, Professors of Radiology, Mayo Clinic College of Medicine. A landmark assessment of the importance of neurovascular anatomy in prostate surgery. Cagri Savas M, Kapucuoglu N, Gursoy K et al 2011 the microvessel density of the hypospadiac prepuce in children. Hinata N, Sejima T, Takenaka A 2013 Progress in pelvic anatomy from the viewpoint of radical prostatectomy. An explanation of the neurological components of bladder function from the higher cortical centres to molecular events within the cells of the detrusor muscle. Orkiszewski M, Madej J 2010 the meatal/urethral width in healthy uncircumcised boys. Stalberg K, Gonzalez R 2012 Urethral atresia and anhydramnios at 18 weeks of gestation can result in normal development. Takahashi T, Ueno M, Azekura K et al 2000 Lateral ligament: its anatomy and clinical importance. Tewari A, Takenaka A, Mtui E et al 2006 the proximal neurovascular plate and the trizonal neural architecture around the prostate gland: importance in the athermal robotic technique of nerve sparing prostatectomy. Yucel S, Guntekin E, Kukul E et al 2004 Comparison of hypospadiac and normal preputial vascular anatomy. Vascular supply and lymphatic drainage the arterial supply to the testis and epididymis is derived from three sources. It covers the tunica vasculosa and is surrounded by the visceral layer of the tunica vaginalis. On the right, it courses anterior to the inferior vena cava and posterior to the middle colic and ileocolic arteries and the terminal ileum. Astherightandlefttesticular arteries enter the pelvis, they lie anterior to the genitofemoral nerves, ureters and external iliac arteries. The cremasteric artery (external spermatic artery) is a branch of the inferior epigastric artery. Suspensory Nerves and vessels exposed by extensive removal of ligament of penis the skin and the superficial fascia of the penis. The skin of the abdomen and parts of the skin of the scrotum have been removed, and the body of the penis has been severed, revealing the internal structure of the penis. The layers of the spermatic cord and the coverings of the testis have been dissected on the right.
Diseases
Sato T medications safe during pregnancy cheap pirfenex 200 mg line, Ito M, Sakamoto H 2013 Pictorial dissection review of the lymphatic pathways from the gallbladder to the abdominal para-aortic lymph nodes and their relationships to the surrounding structures. Singh B, Ramsaroop L, Allopi L et al 2006 Duplicate gallbladder: an unusual case report. Variants were recorded in 20% of patients and predominantly involved the cystic artery (11%), cystic duct (4%), right hepatic artery (3%) and gallbladder (2%). Anatomical variants were associated with a slightly increased incidence of postoperative morbidity. The major part of the gland is exocrine, secreting enzymes involved in the digestion of lipids, carbohydrates and proteins. It has an additional endocrine function derived from clusters of cells scattered throughout the substance of the gland, which take part in glucose homeostasis and the control of upper gastrointestinal motility and function. The healthy pancreas is creamy pink in colour, with a soft to firm consistency and lobulated surface. From about 60 years of age, the gland atrophies and fatty connective tissue replaces exocrine tissue (Caglar et al 2012, Saisho et al 2007). The ventral surface of the pancreas is covered by parietal peritoneum and is crossed by the root of the transverse mesocolon. A loose connective tissue layer immediately posterior to the pancreas, sometimes known the fusion fascia of Treitz in the region of the pancreatic head and the fusion fascia of Toldt in the region of the body and tail, contains vessels that supply the pancreas (Kimura 2000). Posteriorly, the common bile duct is partially embedded within the head of the gland just proximal to where it joins the pancreatic duct near the major duodenal papilla (Burgard et al 1991, Nagai 2003). The posterior surface of the pancreatic head is also related to the inferior vena cava, the right crus of the diaphragm and the termination of the right gonadal vein (Ch. This is a crucial relationship when evaluating pancreatic cancer because malignant involvement of these vessels may make resection impossible. The superior mesenteric vein and portal vein groove the posterior aspect of the neck. The anterior surface of the pancreatic neck is covered by peritoneum and lies adjacent to the pylorus. The anterior superior pancreaticoduodenal branch of the gastroduodenal artery descends in front of the gland at the junction of the head and neck. It is slightly triangular in cross-section, and has anterior and posterior surfaces and superior and inferior borders. It is the thickest and broadest part of the pancreas but is still flattened in the anteroposterior plane. Superiorly, it lies adjacent to the first part of the duodenum; close to the pylorus, however, where the duodenum is on a short mesentery, it overlaps the upper part of the head anteriorly. The duodenal border of the head is flattened, slightly concave and adherent to the second part of the duodenum, particularly around the duodenal papillae.
Muscular branches the muscular branches of the posterior division of the femoral nerve supply quadriceps femoris medicine while pregnant discount pirfenex 200mg otc. A branch to rectus femoris enters its proximal posterior surface and also supplies the hip joint. A larger branch to vastus lateralis forms a neurovascular bundle with the descending branch of the lateral circumflex femoral artery in its distal part and also supplies the knee joint. A branch to vastus medialis descends through the proximal part of the adductor canal, lateral to the saphenous nerve and femoral vessels, and enters the muscle at about its midpoint, sending a long articular filament distally along the muscle to the knee. Two or three branches to vastus intermedius enter its anterior surface about mid-thigh; a small branch from one of these descends through the muscle to supply articularis genus and the knee joint. The posterior branch pierces obturator externus anteriorly, supplies it and passes behind adductor brevis to the front of adductor magnus, dividing into branches to this and adductor brevis when the latter is not supplied by the anterior division. It usually sends an articular filament to the knee joint, which either perforates adductor magnus distally or traverses its opening with the femoral artery to enter the popliteal fossa. Within the fossa, the nerve descends on the popliteal artery to the back of the knee, pierces its oblique posterior ligament and supplies the articular capsule. The nerve may also be damaged by an obturator hernia, or be involved together with the femoral nerve in retroperitoneal lesions that occur close to the origins of the lumbar plexus. A more distal nerve entrapment syndrome causing chronic medial thigh pain has been described in athletes with large adductor muscles. Vascular branches of the femoral nerve supply the femoral artery and its branches. Sometimes the accessory obturator nerve is very small and only supplies pectineus. Any branch may be absent and others may occur; an additional branch sometimes supplies adductor longus. Sciatic nerve the sciatic nerve is 2 cm wide at its origin and is the thickest nerve in the body. Superiorly, it lies deep to gluteus maximus, resting first on the posterior ischial surface with the nerve to quadratus femoris between them. It then crosses posterior to obturator internus, the gemelli and quadratus femoris, separated by the latter from obturator externus and the hip joint. It is accompanied medially by the posterior femoral cutaneous nerve and the inferior gluteal artery. More distally, it lies behind adductor magnus and is crossed posteriorly by the long head of biceps femoris. Its course corresponds to a line drawn from just medial to the midpoint between the ischial tuberosity and greater trochanter to the apex of the popliteal fossa. Articular branches arise proximally to supply the hip joint through its posterior capsule; these are sometimes derived directly from the sacral plexus.
These are termed primary restraints lb 95 medications buy cheap pirfenex 200mg, and are exemplified by the cruciate ligaments and the tibial and fibular collateral ligaments. Secondary restraints are less well aligned but still have a significant restraining effect. With an absent anterior cruciate ligament, the tibial collateral ligament can resist the applied force; however, it does so by being loaded to a much higher level than the original loading on the anterior cruciate ligament. The size of the lines in the vector diagram demonstrate this principle: although joint laxity may remain normal initially following rupture of a primary restraint, it may subsequently result in the overload of a secondary restraint and, ultimately, in further soft tissue failure. The patellofemoral joint is most heavily loaded during weightbearing activities when the knee is flexed. In the frontal plane, quadriceps femoris and the patellar ligament tensions combine to cause a lateralizing force vector termed the Q-angle effect. Clinically, the Q angle is changed by the position of hip rotation, tibial rotation and quadriceps femoris tension. Contraction of quadriceps femoris, therefore, tends to displace the patella laterally, which is resisted by the geometry of the joint and by the ligaments. Vastus medialis obliquus acts medially and posteriorly as much as it acts proximally, and so its tension helps to resist the Q-angle effect. This ligament is the single most important stabilizer of the posterolateral region of the knee and resists lateral rotation of the tibia on the femur. Failure to recognize and reconstruct damage to this ligament and to the related ligamentous structures is the most common reason for a poor result from an otherwise well-performed operation for repair of ruptured cruciate ligaments. Fleshy fibres expand from the inferior limit of the tendon to form a somewhat triangular muscle that descends medially to be inserted into the medial two-thirds of the triangular area above the soleal line on the posterior surface of the tibia, and into the tendinous expansion that covers its surface. An additional head may arise from the sesamoid bone in the lateral head of gastrocnemius. Popliteus minor runs from the posterior surface of the lateral tibial condyle, medial to plantaris, to the oblique popliteal ligament. Peroneotibialis runs deep to popliteus from the medial side of the fibular head to the upper end of the soleal line. Gastrocnemius, plantaris, the popliteal vessels and the tibial nerve all lie posterior to the expansion. The popliteal tendon is intracapsular and is deep to the fibular collateral ligament and the tendon of biceps femoris. It is invested on its deep surface by synovial membrane, and grooves the posterior border of the lateral meniscus and the adjoining part of the tibia before it emerges inferior to the posterior band of the arcuate ligament. There are additional contributions from the nutrient artery of the tibia (from the posterior tibial artery), the proximal part of the posterior tibial artery, and the posterior tibial recurrent artery.
Chromium Acetate (Chromium). Pirfenex.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96895
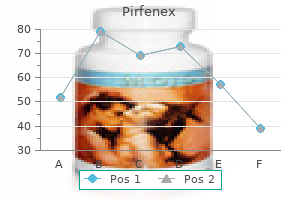
In making such vectorial analy ses medications without a script pirfenex 200 mg online, it should be remembered that the positive end of the injury potential vector points toward the normal cardiac muscle, and the negative end points toward the injured portion of the heart that is emitting the current of injury. This means that the positive end of the vector is in the direction of the anterior chest wall, and the negative end (the injured end of the vector) points away from the chest wall. However, after about 1 week, the injury potential has diminished considerably, and after 3 weeks, it is gone. This is the usual recovery pattern after acute myocardial infarction of moderate degree, showing that the new collateral coronary blood flow develops enough to reestablish appropriate nutrition to most of the infarcted area. In some patients who experience myocardial infarc tion, the infarcted area never redevelops adequate coro nary blood supply. Often, some of the heart muscle dies, but if the muscle does not die, it will continue to show an injury potential as long as the ischemia exists, particularly during bouts of exercise when the heart is overloaded. That is, the T wave becomes abnormal when the normal sequence of repolarization does not occur. The reason for this prolongation is delayed conduction in the left ventricle resulting from left bundle branch block. However, the refrac tory periods of the right and left ventricular muscle masses are not greatly different from each other. Therefore, the right ventricle begins to repolarize long before the left ventricle, which causes strong positivity in the right ven tricle and negativity in the left ventricle at the time that the T wave is developing. These configurations are certainly not found in all cases of old cardiac infarction. Usually, no pain is felt as long as the person is quiet, but as soon as he or she overworks the heart, the pain appears. Instead, the base of the ventricles would repolarize ahead of the apex, and the vector of repolarization would point from the apex toward the base of the heart, opposite to the standard vector of repolarization. Consequently, the T wave in all three standard leads would be negative rather than the usual positive. When the ischemia occurs in only one area of the heart, the depolarization period of this area decreases out of proportion to that in other portions. The ischemia might result from chronic, progressive cor onary occlusion, acute coronary occlusion, or relative coronary insufficiency that occurs during exercise. The changes in the T waves need not be specific because any change in the T wave in any lead-inversion, for instance, or a biphasic wave-is often evidence enough that some portion of the ventricular muscle has a period of depolar ization out of proportion to the rest of the heart, caused by mild to moderate coronary insufficiency. As discussed in Chapter 22, digitalis is a drug that can be used during coronary insufficiency to increase the strength of cardiac muscle contraction. As a result, nonspecific changes, such as Twave inversion or biphasic T waves, may occur in one or more of the electrocardiographic leads. Therefore, changes in the T wave during digitalis administration are often the earliest signs of digitalis toxicity. For instance, sometimes the beat of the atria is not coordinated with the beat of the ventricles, so the atria no longer function as primer pumps for the ventricles. The purpose of this chapter is to discuss the physiology of common cardiac arrhythmias and their effects on heart pumping, as well as their diagnosis by electrocardiography.
Some then pierce the deep fascia to supply the skin medications jokes purchase 200mg pirfenex with visa, while others traverse the interosseous membrane to anastomose with branches of the posterior tibial and fibular arteries. Perforating branches Most of the fasciocutaneous perforators pass along the anterior fibular fascial septum behind extensor digitorum longus before penetrating the deep fascia to supply the skin. Anterior medial malleolar artery the anterior medial malleolar Profunda femoris artery artery arises approximately 5 cm proximal to the ankle. It passes pos terior to the tendons of extensor hallucis longus and tibialis anterior medial to the joint, where it joins branches of the posterior tibial and medial plantar arteries. Anterior lateral malleolar artery the anterior lateral malleolar Femoral artery artery runs posterior to the tendons of extensor digitorum longus and fibularis tertius to the lateral side of the ankle and anastomoses with the perforating branch of the fibular artery and ascending branches of the lateral tarsal artery. It descends medially in the flexor compartment and divides under abductor hal lucis, midway between the medial malleolus and the calcaneal tubercle, into the medial and lateral plantar arteries. The artery may be much reduced in length or in calibre; the fibular artery then takes over its distal territory of supply and may consequently be increased in size. Anterior tibial artery Posterior tibial artery Relations the named branches of the posterior tibial artery are the circumflex fibular, nutrient, muscular, perforating, communicating, medial malle olar, calcaneal, lateral and medial plantar, and fibular arteries. Proximally, gas trocnemius, soleus and the transverse intermuscular septum of the leg are superficial to the artery, and distally, it is covered only by skin and fascia. The nerve is at first medial to the artery but soon crosses behind it and subsequently becomes largely posterolateral in position. Reaching the inferior tibiofibular syn desmosis, it divides into calcaneal branches that ramify on the lateral and posterior surfaces of the calcaneus. Proximally, it is covered by soleus and the transverse intermuscular septum between soleus and the deep muscles of the leg, and distally it is overlapped by flexor hallucis longus. It may also branch more distally from the posterior tibial artery, sometimes 7 or 8 cm distal to popliteus. Its size tends to be inversely related to the size of the other arteries of the leg. It may be reduced in size but is more often enlarged, when it may join, reinforce or even replace the posterior tibial artery in the distal leg and foot. Nutrient artery of the tibia the nutrient artery of the tibia arises from the posterior tibia near its origin. After giving off a few muscular branches, it descends into the bone immediately distal to the soleal line. Muscular branches Muscular branches are distributed to the soleus and deep flexors of the leg. Perforating branches Approximately five fasciocutaneous perfor ators emerge between flexor digitorum longus and soleus, and pass through the deep fascia, often accompanying the perforating veins that connect the deep and superficial venous systems.

Baroreceptor Arterial Pressure Control System-Baroreceptor Reflexes By far the best known of the nervous mechanisms for arterial pressure control is the baroreceptor reflex medications used to treat migraines 200mg pirfenex visa. Basically, this reflex is initiated by stretch receptors, called either baroreceptors or pressoreceptors, located at specific points in the walls of several large systemic arteries. Note that the carotid sinus barore ceptors are not stimulated at all by pressures between 0 and 50 to 60 mm Hg, but above these levels, they respond progressively more rapidly and reach a maximum at about 180 mm Hg. The responses of the aortic baroreceptors are similar to those of the carotid receptors except that they operate, in general, at arterial pressure levels about 30 mm Hg higher. Note especially that in the normal operating range of arterial pressure, around 100 mm Hg, even a slight change in pressure causes a strong change in the barore flex signal to readjust arterial pressure back toward normal. Thus, the baroreceptor feedback mechanism functions most effectively in the pressure range where it is most needed. The baroreceptors respond rapidly to changes in arte rial pressure; in fact, the rate of impulse firing increases in the fraction of a second during each systole and decreases again during diastole. Furthermore, the barore ceptors respond much more to a rapidly changing pressure than to a stationary pressure. That is, if the mean arterial pressure is 150 mm Hg but at that moment is rising rapidly, the rate of impulse transmission may be as much as twice that when the pressure is stationary at 150 mm Hg. The net effects are (1) vasodilation of the veins and arterioles throughout the peripheral circulatory system and (2) decreased heart rate and strength of heart contraction. Therefore, excita tion of the baroreceptors by high pressure in the arteries reflexly causes the arterial pressure to decrease because of 220 both a decrease in peripheral resistance and a decrease in cardiac output. Conversely, low pressure has opposite effects, reflexly causing the pressure to rise back toward normal. This reduces the carotid sinus pressure; as a result, signals from the baroreceptors decrease and cause less inhibitory effect on the vasomotor center. The vaso motor center then becomes much more active than usual, causing the aortic arterial pressure to rise and remain elevated during the 10 minutes that the carotids are occluded. Removal of the occlusion allows the pressure in the carotid sinuses to rise, and the carotid sinus reflex now causes the aortic pressure to fall immediately to slightly below normal as a momentary overcompensation and then return to normal in another minute. The Baroreceptors Attenuate Blood Pressure Changes During Changes in Body Posture. Immediately on standing, the arterial pressure in the head and upper part of the body tends to fall, and marked reduction of this pressure could cause loss of consciousness. However, the falling pressure at the baroreceptors elicits an immediate reflex, resulting in strong sympathetic discharge through out the body that minimizes the decrease in pressure in the head and upper body.
Ventricular fibrillation results from cardiac impulses that have gone berserk within the ventricular muscle mass treatment tinnitus pirfenex 200mg visa, stimulating first one portion of the ventricular muscle, then another portion, then another, and eventually feeding back onto itself to re-excite the same ventricular muscle over and over, never stopping. When this phenomenon occurs, many small portions of the ventricular muscle will be contracting at the same time, while equally as many other portions will be relaxing. Thus, there is never a coordinated contraction of all the ventricular muscle at once, which is required for a pumping cycle of the heart. Despite massive movement of stimulatory signals throughout the ventricles, the ventricular chambers neither enlarge nor contract but remain in an indeterminate stage of partial contraction, pumping either no blood or negligible amounts. Therefore, after fibrillation begins, unconsciousness occurs within 4 to 5 seconds because of lack of blood flow to the brain, and irretrievable death of tissues begins to occur throughout the body within a few minutes. Multiple factors can spark the beginning of ventricular fibrillation; a person may have a normal heartbeat one moment, but 1 second later, the ventricles are in fibrillation. Especially likely to initiate fibrillation are (1) sudden electrical shock of the heart or (2) ischemia of the heart muscle, of its specialized conducting system, or both. Therefore, that impulse dies, and the heart awaits a new action potential to begin in the atrial sinus node. Therefore, let us explain more fully the background conditions that can initiate re-entry and lead to "circus movements," which in turn cause ventricular fibrillation. If the originally stimulated muscle fibers are still in a refractory state, the impulse then dies out because refractory muscle cannot transmit a second impulse. Circus movement, showing annihilation of the impulse in the short pathway and continued propagation of the impulseinthelongpathway. By this time, the originally stimulated muscle might be out of the refractory state, and the impulse can continue around the circle again and again. All these conditions occur in different pathological states of the human heart, as follows: (1) A long pathway typically occurs in dilated hearts. Thus, in many cardiac disturbances, re-entry can cause abnormal patterns of cardiac contraction or abnormal cardiac rhythms that ignore the pace-setting effects of the sinus node. Instead, they have degenerated into a series of multiple wave fronts that have the appearance of a chain reaction. One of the best ways to explain this process in fibrillation is to describe the initiation of fibrillation by electric shock with a 60-cycle alternating electric current. The first cycle of the electrical stimulus causes a depolarization wave to spread in all directions, leaving all the muscle beneath the electrode in a refractory state. This state of events is depicted in heart A by many lighter patches, which represent excitable cardiac muscle, and dark patches, which represent muscle that is still refractory. Now, continuing 60-cycle stimuli from the electrode can cause impulses to travel only in certain directions through the heart but not in all directions. Thus, in heart A, certain impulses travel for short distances until they reach refractory areas of the heart, and then they are blocked. However, other impulses pass between the refractory areas and continue to travel in the excitable areas.

As Acute Pulmonary Edema in LateStage Heart Failure-Another Lethal Vicious Cycle A frequent cause of death is acute pulmonary edema occurring in patients who have already had heart failure for a long time treatment 2 cheap pirfenex 200 mg otc. When acute pulmonary edema occurs in a person without new cardiac damage, it usually is set off by some temporary overload of the heart, such as might result from a bout of heavy exercise, an emotional experience, or even a severe cold. The acute pulmonary edema is believed to result from the following vicious cycle: 1. A temporarily increased load on the already weak left ventricle initiates the vicious cycle. Because of limited pumping capacity of the left heart, blood begins to dam up in the lungs. The increased blood in the lungs elevates the pulmonary capillary pressure, and a small amount of fluid begins to transude into the lung tissues and alveoli. The increased fluid in the lungs diminishes the degree of oxygenation of the blood. The decreased oxygen in the blood further weakens the heart and also causes peripheral vasodilation. The peripheral vasodilation further increases venous return of blood from the peripheral circulation. The increased venous return further increases the damming of the blood in the lungs, leading to still long as persons with low cardiac reserve remain in a state of rest, they usually will not experience major symptoms of heart disease. However, a diagnosis of low cardiac reserve usually can be made by requiring the person to exercise either on a treadmill or by walking up and down steps, either of which requires greatly increased cardiac output. Immediate and sometimes extreme shortness of breath (dyspnea) resulting from failure of the heart to pump sufficient blood to the tissues, thereby causing tissue ischemia and creating a sensation of air hunger 2. An excessive increase in heart rate because the nervous reflexes to the heart overreact in an attempt to overcome the inadequate cardiac output Exercise tests are part of the armamentarium of the cardiologist. These tests take the place of cardiac output measurements that cannot be made with ease in most clinical settings. During the first few seconds after a moderately severe heart attack, the cardiac output curve falls to the lowermost curve. During these few seconds, the venous return curve still has not changed because the peripheral circulatory system is still operating normally. Therefore, the new state of the circulation is depicted by point B, where the new cardiac output curve crosses the normal venous return curve. Thus, the right atrial pressure rises immediately to 4 mm Hg, whereas the cardiac output falls to 2 L/min. One such approach is the graphical method for analysis of cardiac output regulation introduced in Chapter 20.
Kippler, 41 years: Under rarer conditions, a place in the atrial or ventricular muscle develops excessive excitability and becomes the pacemaker. If it is inadvertently retained in utero after delivery of the main placental mass, it can cause postpartum haemorrhage or infection. The total conductance (Ctotal) for blood flow is the sum of the conductance of each parallel pathway: C total = C1 + C2 + C3 + C 4. B, Variations in the number and patterns of branching of the renal artery (percentages are approximate).
Angir, 55 years: Sholten et al (2013) reported variant suprarenal veins in 13% of individuals undergoing laparoscopic adrenalectomy, more often on the right (17%) than the left (9%). It pierces the oblique popliteal ligament to supply the cruciate ligaments and synovial membrane. A branch of the nerve to popliteus (tibial nerve) supplies the posterior portion of the superior tibiofibular joint. Finally, the A-V valves are supported by the chordae tendineae, which is not true for the semilunar valves.
Grok, 64 years: Spontaneous hereditary hypertension has been observed in several strains of animals, including different strains of rats, rabbits, and at least one strain of dogs. These factors can all be expressed quantitatively by the venous return curve, as we explain in the next sections. Electrodes Lack of blood flow to the brain for more than 5 to 8 minutes usually causes permanent mental impairment or even destruction of brain tissue. The profunda femoris artery, obturator artery and femoral artery all contribute; the main supply comes directly from the distal part of the profunda femoris artery.
Goran, 38 years: Branches In addition to the external iliac and internal iliac branches, each common iliac artery also gives small branches to the peritoneum, psoas major, ureter, adjacent nerves and surrounding areolar tissue. In a normal heart, almost no large communications exist among the larger coronary arteries. The two pubic bones articulate anteriorly at the pubic symphysis and the sacrum articulates posteriorly with the two iliac bones at the sacroiliac joint; the bones are virtually incapable of independent movement, except in the female during parturition or as a result of pathological change. It normally increases in size from 10 mm in diameter to 25 mm at 8 weeks of gestation and can be seen clearly on ultrasound.
References