




Hermann Einsele
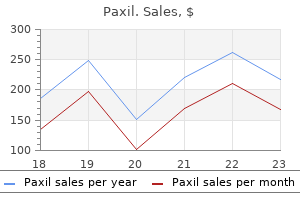
Paxil dosages: 40 mg, 30 mg, 20 mg, 10 mg
Paxil packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 360 pills, 270 pills

Treadmill exercise electrocardiography is inexpensive and available at many hospitals every day symptoms when quitting smoking cheap 30 mg paxil free shipping, beyond traditional laboratory hours, and prospective data indicate that early exercise test results provide reliable prognostic information for low-risk patient populations. Analyses of pooled data have suggested that the prevalence of coronary disease in populations undergoing early exercise testing averages approximately 5%, and that the rate of adverse events is negligible. Imaging studies are less readily available and more expensive than exercise electrocardiography but have increased sensitivity for the detection of coronary disease and the ability to quantify the extent of and localize jeopardized myocardium. High-risk rest perfusion scans are associated with an increased risk for major cardiac complications, whereas patients with low-risk scans have low 30-day cardiac event rates (<2%). Rest myocardial perfusion imaging is most sensitive if performed when a patient is experiencing ischemic symptoms, with its sensitivity progressively diminishing thereafter. Imaging should be performed within 2 hours of the resolution of symptoms, although data support its use for up to 4 hours. Echocardiography can also be used, with and without stress, to detect wall motion abnormalities consistent with myocardial ischemia. The presence of induced or baseline regional wall motion abnormalities correlates with a worse prognosis. The sensitivity of stress echocardiography appears to be comparable to that of myocardial perfusion imaging (85% to 90%), and its specificity is somewhat better (80% to 95% versus 75% to 90%). The addition of T2-weighted imaging, which can detect myocardial edema and thus help differentiate acute from chronic perfusion defects, improves the specificity to 96% without sacrificing sensitivity. The remaining 50% had evidence of atherosclerosis, with 32% having minor plaque and 18% having a stenosis greater than 50%. Keller T, Zeller T, Peetz D, et al: Sensitive troponin I assay in early diagnosis of acute myocardial infarction. Reiter M, Twerenbold R, Reichlin T, et al: Early diagnosis of acute myocardial infarction in patients with pre-existing coronary artery disease using more sensitive cardiac troponin assays. Reichlin T, Irfan A, Twerenbold R, et al: Utility of absolute and relative changes in cardiac troponin concentrations in the early diagnosis of acute myocardial infarction. Lockie T, Nagel E, Redwood S, Plein S: Use of cardiovascular magnetic resonance imaging in acute coronary syndromes. Yang Q, Li K, Liu X, et al: Contrast-enhanced whole-heart coronary magnetic resonance angiography at 3. Characteristic findings include coagulation necrosis and contraction band necrosis, often with patchy areas of myocytolysis at the periphery of the infarct. The "coronary care unit phase" began in the mid-1960s and emphasized early detection and management of cardiac arrhythmias based on the development of monitoring and cardioversion/defibrillation capabilities.
Even though most patients with aortic dissection will have abnormal findings on a chest radiograph treatment goals for depression purchase 10 mg paxil with visa, 12% to 15% have chest radiographs with normal findings. Thus normal chest radiograph results cannot exclude the presence of an aortic dissection. The electrocardiographic findings in patients with aortic dissection are nonspecific but may indicate acute complications such as myocardial ischemia or infarction related to coronary artery 1292. There is malcoaptation of the aortic valve leaflets because of aortic root and annular dilation. The presence of acute coronary ischemia is particularly dangerous because it may lead the clinician away from the evaluation of dissection. Reliable biomarkers for the diagnosis or exclusion of acute aortic dissection have aroused great interest. Although a negative D-dimer result in low-suspicion patients may be useful, the negative likelihood ratio provided by the D-dimer assay is not sufficient in high-risk individuals and cannot "rule out" the disease in these patients. First, it is contraindicated in patients with certain implantable devices (pacemaker, defibrillator) and other metallic implants. Echocardiography the echocardiographic finding considered diagnostic of aortic dissection is the presence of an undulating intimal flap within the aortic lumen that separates the true and false channels (Videos 57-8 to 57-12; also see Videos 57-4 and 57-6). Reverberations and other artifacts can cause linear echodensities within the aortic lumen that mimic aortic dissection. Differing from such artifacts, a dissection flap has motion independent of the surrounding structures and is contained within the aortic lumen. In cases in which the false lumen is thrombosed, displacement of intimal calcification or thickening of the aortic wall may suggest aortic dissection. DiagnosticTechniques When aortic dissection is suspected, quick and accurate confirmation of the diagnosis is important. If the probability of dissection is very high and initial testing is negative or nondiagnostic, a second diagnostic test should be performed. When comparing imaging modalities, one must consider the diagnostic information needed (Table e57-3). Besides diagnosing the type and location of dissection, additional useful information includes anatomic features and complications related to the dissection, including its extent, entry sites, and reentry sites; patency of the false lumen; involvement of branch vessels; severity of aortic regurgitation; hemopericardium; coronary artery involvement; malperfusion; and rupture or leaking. Linear reverberation artifacts are common, particularly in a dilated ascending aorta, and may be mistaken for a dissection flap. The intimal flap is visualized just distal to the aortic valve and extending distally.
Syndromes
If a patient has structural heart disease symptoms als order 10 mg paxil with mastercard, other cardiovascular causes of syncope should be excluded before considering a positive response to upright tilt testing to be diagnostic of neurally mediated syncope. Upright tilt testing is also indicated in the evaluation of patients for whom the cause of the syncope has been determined. Upright tilt testing has no value in assessing the efficacy of treatment of neurally mediated syncope. Tilt-TableTesting Myocardial ischemia is an unlikely cause of syncope and, when present, is usually accompanied by angina (see Chapter 49). The use of stress tests (see Chapter 13) is best reserved for patients in whom syncope or presyncope occurred during or immediately after exertion in association with chest pain or in a patient at high risk for coronary artery disease. In contrast, syncope following exercise is usually caused by neurally mediated syncope. Even in patients with syncope during exertion, exercise stress testing is highly unlikely to trigger another event. Coronary angiography is recommended in patients with syncope suspected to be due, directly or indirectly, to myocardial ischemia. Despite the low diagnostic yield of electrocardiography, the test is inexpensive and risk free and is considered a standard part of the evaluation of virtually all patients with syncope. However, because of the infrequent and sporadic nature of syncope, the diagnostic yield of Holter monitoring in the evaluation of patients with syncope and presyncope is extremely low. Holter monitoring and inpatient telemetry monitoring are most likely to be diagnostic when Echocardiograms are commonly used to evaluate patients with syncope, but current guidelines suggest that an echocardiogram should be performed only in patients suspected of having structural heart disease. Echocardiographic findings considered diagnostic of the cause of syncope include severe aortic stenosis, pericardial tamponade, aortic dissection, congenital abnormalities of the coronary arteries, and obstructive atrial myxomas or thrombi. Findings of impaired right or left ventricular function, evidence of right ventricular overload or pulmonary hypertension (pulmonary emboli), or the presence of hypertrophic cardiomyopathy (see Chapter 66) are of prognostic importance and justify additional diagnostic testing. A recent advancement in this technology is that these implantable event monitors can be accessed by remote monitoring, 40 which further increases their diagnostic effectiveness. Continuous-loop event monitors, often programmed with 5 to 15 minutes of preactivation memory stored by the device, are preferred because the data can be retrieved for analysis. Prospective event monitors not worn continuously by the patient are of value to investigate palpitations but play no role in the evaluation of patients with syncope. Event monitors are indicated in the early phase of the evaluation of patients with syncope of uncertain origin who do not have high-risk criteria that require immediate hospitalization or intensive evaluation. They are also indicated in high-risk patients in whom a comprehensive evaluation did not demonstrate a cause of the syncope or lead to specific treatment. Studies have demonstrated that these devices result in higher diagnostic yield in patients with syncope or presyncope than do the conventional event monitors just described. Modified from Moya A, Sutton R, Ammirati F, et al: Guidelines for the diagnosis and management of syncope 2009. In addition, programmed electrical stimulation via standard techniques should be performed to evaluate the inducibility of ventricular and supraventricular arrhythmias.

All pacing and defibrillation in implantable devices result from discharge of a capacitor treatment 0f ovarian cyst 10 mg paxil buy with amex. The strength-duration curve can be approximated by an inverse exponential or hyperbolic function. The rheobase is the longduration asymptote (essentially the lowest value), which is determined by properties of the lead system and electrode-myocardial interface. The chronaxie is the duration at which the threshold is twice the rheobase amplitude. It may be considered an approximation of an aggregate membrane time constant for the myocardium. A waveform with a duration approximately equal to the chronaxie paces with the lowest energy. Presently, no comprehensive theory permits determining the waveform duration that defibrillates with lowest energy from first principles, but approximations and empiric data relate it to the chronaxie. For capacitive-discharge defibrillation waveforms, the duration (of the first phase of a biphasic waveform) that defibrillates with minimum energy may be considered intermediate between the optimal duration for response of the cell membrane (chronaxie or m) and the optimal duration for the capacitor to deliver its charge (w). Usually, w exceeds m, so phase 1 of transvenous biphasic waveforms exceeds the chronaxie by 25% to 75%. All pacing and defibrillation waveforms in implantable devices have capacitive-discharge waveforms with a fixed leading-edge voltage and a trailing-edge voltage determined by the waveform duration and time constant w. B, Monophasic truncated exponential waveform with initial voltage Vi and final voltage Vf. In comparison to the pacing waveform, the voltage is approximately 100 times greater and the duration is approximately 10 times greater. C, Biphasic truncated exponential waveform with initial voltage of the second phase, V i (2), equal to the final voltage of the first phase, Vf (1). Signals that do not originate in the local myocardium are called far-field signals. T waves have a lower frequency (1 to 10 Hz), whereas most noncardiac myopotentials and electromagnetic interference have higher frequencies. The ability of the heart rate to increase during exertion is termed chronotropic competence. Lower safety margins may be programmed for pacemakers that determine capture automatically on a beat-to-beat basis. At the long coupling intervals used for bradycardia pacing, the pacing threshold is lower if the negative electrode (cathode) is used for stimulation, but at short coupling intervals, which may initiate tachyarrhythmias, the stimulation threshold is lower for the positive electrode (anode). Anodal stimulation of the right ventricular defibrillation electrode is preferred for defibrillation, although polarity has little effect on the efficacy of defibrillation for presently used biphasic defibrillation waveforms. The most clinically important metabolic abnormality is hyperkalemia, which raises pacing and defibrillation thresholds and alters sensing by causing conduction delays and local conduction block. Additionally, marked acidosis or alkalosis raises pacing thresholds but does not affect defibrillation thresholds. However, in common use, the terms unipolar and bipolar refer to the number of intracardiac electrodes in the recording electrode pair.

Intracardiac or transesophageal defibrillation can be tried if electrical cardioversion of patients with atrial fibrillation can revert all attempts at external cardioversion fail medicine clipart paxil 40 mg order visa. All equipment necessary for emergency resuscitation should be immediately accessible. Before cardioversion, 100% oxygen may be administered for 5 to 15 minutes by nasal cannula or facemask and is continued throughout the procedure. Manual ventilation of the patient may be necessary to avoid hypoxia during periods of deepest sedation. Adequate sedation of the patient undergoing even urgent cardioversion is essential. In up to 5% of patients with atrial fibrillation, sinus rhythm cannot be restored by external countershock despite all the preceding measures, including ibutilide pretreatment and biphasic shocks. It is important to distinguish between inability to attain sinus rhythm, indicating inadequate delivery of energy to the atria, and inability to maintain sinus rhythm after transient termination of fibrillation; the latter condition (early reinitiation of atrial fibrillation) does not respond to higherenergy shocks because fibrillation has already been terminated but quickly recurs. Pretreatment with an antiarrhythmic drug may help maintain sinus rhythm after subsequent shocks. Patients in whom atrial fibrillation simply cannot be terminated with an external shock tend to be very obese or have severe obstructive lung disease. In such cases, internal cardioversion can be performed with the use of specially configured catheters that have multiple large electrodes covering several centimeters of the distal portion of the catheter for distributing the shock energy. By standard percutaneous access, these catheters can be situated in the lateral part of the right atrium and coronary sinus to achieve a shock vector across most of the atrial mass. With such configurations, internal shocks of 2 to 15 J can terminate atrial fibrillation in more than 90% of patients whose arrhythmia is refractory to transthoracic shock. Indications As a rule, any nonsinus tachycardia that produces hypotension, congestive heart failure, mental status changes, or angina and does not respond promptly to medical management should be terminated electrically. Very rapid ventricular rates in patients with atrial fibrillation and Wolff-Parkinson-White syndrome are often best treated by electrical cardioversion. Rarely, a patient may experience hypotension, reduced cardiac output, or congestive heart failure after the shock. This problem may be related to complications of the cardioversion, such as embolic events, myocardial depression resulting from the anesthetic agent or the shock itself, hypoxia, lack of restoration of left atrial contraction despite return of electrical atrial systole, or postshock arrhythmias. Direct-current countershock of digitalis-induced tachyarrhythmias is contraindicated. In patients who have indications for chronic warfarin therapy to prevent stroke, the hope of avoiding anticoagulation by restoring sinus rhythm is not a reason to attempt cardioversion because these patients are still at increased risk for thromboembolic events. Several large trials have shown that maintenance of sinus rhythm confers no survival advantage over rate control and anticoagulation; thus, not all patients with newly discovered atrial fibrillation warrant an attempt at restoration of sinus rhythm. Unfavorable candidates include patients with (1) digitalis toxicity; (2) no symptoms and a well-controlled ventricular rate without therapy; (3) sinus node dysfunction and various unstable supraventricular tachyarrhythmias or bradyarrhythmias-often bradycardiatachycardia syndrome-in whom atrial fibrillation finally develops and is maintained, which in essence represents a cure for sick sinus syndrome; (4) little or no symptomatic improvement with normal sinus rhythm who promptly revert to atrial fibrillation after cardioversion despite drug therapy; (5) a large left atrium and longstanding atrial fibrillation; (6) episodes of atrial fibrillation that revert 35 spontaneously to sinus rhythm; (7) no mechanical atrial systole after the return of electrical atrial systole; (8) atrial fibrillation and advanced heart block; (9) cardiac surgery planned in the near future; and (10) antiarrhythmic drug intolerance. Atrial fibrillation is more likely to recur after cardioversion in patients who have significant chronic obstructive lung disease, congestive heart failure, mitral valve disease (particularly mitral regurgitation), atrial fibrillation present longer than 1 year, and an enlarged left atrium (echocardiographic diameter larger than 4.
High-frequency components of R-R interval With other systems treatment jerawat di palembang 40 mg paxil for sale, the device automatically begins recording the variability reflect tonic vagal activity. Reduced R-R interval variability, rhythm when the heart rate increases or decreases outside preset a marker of increased risk, indicates loss or reduction of the physioparameters. Some systems incorporate cell phone technology that logic periodic sinus node fluctuations, which has many potential automatically notifies a central monitoring facility when certain concauses and may not necessarily represent a significant shift in autoditions are met. New indices of heart rate variability are continually the time between occurrence and effective treatment of serious being evaluated. Even the simple measure of resting heart rate has arrhythmias can be significantly shortened. Heart rate turbulence is a measure of reflex vagal control of the heart, whereas heart rate variability is more indicative of overall vagal tone. Abnormal heart rate turbulence is a strong independent predictor of mortality in patients with coronary artery disease and dilated cardiomyopathy; abnormal indices in some patients can be improved or normalized after treatment with beta blockers and statin drugs. Different techniques exist for determining dispersion (including automated algorithms), and the results of one study are often difficult to compare with those of another; in addition, the test is sensitive to age, time of day, season of year, and even body position. Signal-Averaged Electrocardiography and Late Potentials Signal averaging is a method that improves the signal-to-noise ratio when the signals are recurrent and the noise is random. In conjunction with appropriate filtering and other methods of noise reduction, signal averaging can detect cardiac signals of a few microvolts in amplitude and reduce noise amplitude, such as muscle potentials, which are typically 5 to 25 mV, to less than 1 mV. One constituent of reentrant ventricular arrhythmias in patients with previous myocardial damage is slow conduction. Signal averaging has been applied clinically most often to detect such late ventricular potentials of 1 to 25 mV. Late potentials can be detected as early as 3 hours after the onset of coronary artery occlusion, increase in prevalence in the first week after myocardial infarction, and disappear in some patients after 1 year. The presence of a late potential is a sensitive but not specific marker of arrhythmic risk, and therefore its prognostic use is limited. The high-pass filtering used to record late potentials meeting the criteria just noted is called time domain analysis because the filter output corresponds in time to the input signal. Some data suggest that frequency domain analysis provides useful information not available with time domain analysis. The electrophysiologic basis appears to be the alternation of repolarization of ventricular myocytes. T wave alternans testing requires exercise or atrial pacing to achieve a heart rate of 100 to 120 beats/min with relatively little atrial or ventricular ectopic activity. Both frequency domain (spectral method) and time domain (modified moving average) analyses have usefulness in risk stratification.
Golden Daisy (Ox-Eye Daisy). Paxil.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96106
Mechanical mechanisms include rupture of the ventricle medications in pregnancy generic 40 mg paxil, cardiac tamponade, acute mechanical obstruction to flow, and acute disruption of a major blood vessel. Closely related to the potential for successful resuscitation is the decision regarding whether to attempt to resuscitate. Although 41% of the patients had suffered an acute myocardial infarction, 73% had a history of congestive heart failure and 20% had experienced previous cardiac arrests. The mean age of 70 years may have influenced the outcome statistics, but patients with high-risk complicated myocardial infarction and those with other high-risk markers heavily influenced the population of patients at risk for in-hospital cardiac arrest. Adverse risks were age older than 70 years, previous stroke or renal failure, and heart failure on admission. Better outcomes were predicted by previous angina pectoris or admission because of ventricular arrhythmias. Strategic factors affecting survival after in-hospital cardiac arrest include the location in the hospital, the type of hospital, daytime and evening events versus night and weekend events, and a rapid time to performance of defibrillation. However, the proportion maintained on mechanical ventilators at the time of arrest did increase from 67. The fraction of out-of-hospital cardiac arrest survivors who are discharged from the hospital alive may now equal or exceed the fraction of in-hospital cardiac arrest victims who are discharged alive, and the postdischarge mortality rate for in-hospital cardiac arrest survivors is higher than that for out-of-hospital cardiac arrest survivors; these are telling clinical statistics. They emphasize the success of preventive measures for cardiac arrest in low-risk in-hospital patients, a finding indicating that these statistics are dominated by higher risk patients. However, other data demonstrate that survival after in-hospital cardiac arrest is lower for events that occur during weeknights and weekends than during the daytime and evening hours during the week125 and that more rapid times to defibrillation are advantageous. Among elderly persons, outcomes after community-based responses to out-of-hospital cardiac arrest are not as good as for younger victims. In one study comparing persons younger than 80 years (mean age, 64 years) with those in their 80s and 90s, the survival rate to hospital discharge in the younger group was 19. ArrhythmiAs, sudden deAth, And syncope 17%, respectively), but the frequency of ventricular tachyarrhythmias versus nonshockable rhythms was lower in elderly persons. Overall, advanced age is only a weak predictor of an adverse outcome and should not be used in isolation as a reason to not resuscitate. Longterm neurologic status and length of hospitalization were similar in older and younger surviving patients. ProgressiontoBiologicDeath the time course for progression from cardiac arrest to biologic death is related to the mechanism of the cardiac arrest, the nature of the underlying disease process, and the delay between onset and resuscitative efforts.

Flecainide exhibits marked usedependent depressant effects on the rapid sodium channel by decreasing Vmax and has slow onset and offset kinetics (see Tables 35-1 treatment 02 bournemouth discount paxil 30 mg overnight delivery, 35-2, 35-3, and 35-5). Drug dissociation from the sodium channel is slow, with time constants of 10 to 30 seconds (versus 4 to 8 seconds for quinidine and less than 1 second for lidocaine). Flecainide shortens the duration of the Purkinje fiber action potential but prolongs it in ventricular muscle, actions that depending on the circumstances, could enhance or reduce electrical heterogeneity and create or suppress arrhythmias. Flecainide profoundly slows conduction in all cardiac fibers and, in high concentrations, inhibits the slow Ca2+ channel (see Chapter 33). Anterograde and retrograde refractoriness in accessory pathways can increase significantly in a use-dependent fashion. Sinus node function remains unchanged in normal subjects but may be depressed in patients with sinus node dysfunction. Flecainide can facilitate or inhibit reentry and may transform atrial fibrillation to flutter. Pacing and defibrillation thresholds are characteristically slightly to significantly increased. Flecainide depresses cardiac performance, particularly in patients with compromised ventricular systolic function, and should be used cautiously or not at all in those with moderate or severe ventricular systolic dysfunction. Flecainide is at least 90% absorbed, with peak plasma concentrations being achieved in 3 to 4 hours. Its elimination half-life in patients with ventricular arrhythmias is 20 hours, with 85% of the drug being excreted unchanged or as an inactive metabolite in urine (see Table 35-4). Elimination is slower in patients with renal disease and heart failure, and doses should be reduced in these situations. Increases in serum concentrations of digoxin (15% to 25%) and propranolol (30%) result during coadministration with flecainide. Propranolol, quinidine, and amiodarone may increase flecainide serum concentrations. Five to 7 days of dosing may be required to reach a steady-state concentration in some patients. ArrhythmiAs, sudden deAth, And syncope Phenytoin Phenytoin was used originally to treat seizure disorders. Phenytoin effectively abolishes abnormal automaticity caused by digitalis-induced delayed afterdepolarizations in cardiac Purkinje fibers and suppresses certain digitalisinduced arrhythmias in humans (see Tables 35-1, 35-2, 35-3, and 35-5). The rate of rise of action potentials initiated early in the relative refractory period is increased, as is membrane responsiveness, which possibly reduces the chance of impaired conduction and block. It has no peripheral cholinergic- or beta-adrenergic blocking actions and minimal hemodynamic effect.

Most adults with preexcitation syndrome have normal hearts symptoms 3 months pregnant 30 mg paxil order fast delivery, although various acquired and congenital cardiac defects have been reported, including Ebstein anomaly, mitral valve prolapse, and cardiomyopathies. Patients with Ebstein anomaly (see Chapter 62) often have multiple right-sided accessory pathways, either in the posterior septum or in the posterolateral wall, with preexcitation localized to the atrialized ventricle. The anomalous complexes can mask or mimic myocardial infarction (see Chapter 51), bundle branch block, or ventricular hypertrophy, and the presence of preexcitation syndrome can suggest an associated cardiac defect. For most patients with recurrent tachycardia, the prognosis is good, but sudden death does occur rarely, with an estimated frequency of 0. Relatives of patients with preexcitation, particularly those with multiple pathways, have an increased prevalence of preexcitation, thus suggesting a hereditary mode of acquisition. Some children and adults can lose their tendency for the development of tachyarrhythmias as they grow older, possibly as a result of fibrotic or other changes at the site of insertion of the accessory pathway. Tachycardia still present after 5 years of age persists in 75% of patients, regardless of the location of the accessory pathway. Intermittent preexcitation during sinus rhythm and abrupt loss of conduction over the accessory pathway after intravenous administration of procainamide and with exercise suggest that the refractory period of the accessory pathway is long and that the patient is not at risk for a rapid ventricular rate should atrial flutter or fibrillation develop. These approaches are relatively specific but not very sensitive, with low positive predictive accuracy. After vagal maneuvers, adenosine followed by intravenous verapamil or diltiazem is the initial treatment of choice. Atrial fibrillation can occur after drug administration, particularly adenosine, along with a rapid ventricular response. An external cardioverterdefibrillator should be immediately available if necessary. In many patients, particularly those with a very rapid ventricular response and any signs of hemodynamic impairment, electrical cardioversion is the initial treatment of choice. For patients with frequent symptomatic arrhythmias that are not fully controlled by drugs, those who are drug intolerant, or those who do not wish to take drugs, ablation is advisable. This option should be considered early in the course of treatment of a symptomatic patient because of its high success rate, low frequency of complications, and potential cost-effectiveness. Ablation is the treatment of choice in patients with atrial fibrillation and rapid conduction over an accessory pathway. Even though transvenous catheter ablation is generally very effective, epicardial ablation through a pericardial approach or surgical interruption of the accessory pathway may be necessary in rare cases. Drug therapy is an alternative to ablation, but it is not always possible to predict which drugs may be most effective for an individual patient. Oral administration of two drugs, such as flecainide and propranolol, to decrease conduction capability in both limbs of the reentrant circuit can be beneficial. For patients who have atrial fibrillation with a rapid ventricular response, induction of atrial fibrillation while the patient is receiving therapy is essential to be certain that the ventricular rate is controlled.
Extensive xanthoma formation on the face and palmar areas can result from accumulation of lipoprotein-x symptoms 2 days before period generic paxil 40 mg buy line. Bile Acid Absorption Inhibitors Cholestyramine Colestipol Colesevelam Questran Colestid WelChol 2-24 g 5-30 g 3. Cholesterol Absorption Inhibitors Ezetimibe Fibrates* Bezafibrate Fenofibrate Gemfibrozil Niacin Zetia (Ezetrol) 10 mg Medication Several medications can alter lipoproteins. Retinoic acid and estrogens can increase triglyceride levels, sometimes dramatically. The exact composition, dosage, and frequency of use of anabolic steroids are often impossible to gather from the patient. The use of second-generation antipsychotic medications may lead to metabolic disorders, weight gain, and lipoprotein abnormalities. Lifestyle changes (diet, exercise, reduction of abdominal obesity) should form the foundation for the treatment of most dyslipidemias. The effects of marked alterations in lifestyle, reduction in dietary fats, especially saturated fats, and exercise can improve cardiovascular risk factors. Rigorous clinical data showing that these measures improve outcomes and implementing them in a sustained manner in practice, however, have proved more difficult. Cholestyramine (Questran) is used in 4-g unit doses as a powder, and colestipol (Colestid) is used in 5-g unit doses. The most important side effects are predominantly gastrointestinal: constipation, a sensation of fullness, and gastrointestinal discomfort. Colesevelam can also decrease glycated hemoglobin A1c (HbA1c), thus making this drug a potentially useful adjunct in the treatment of complicated diabetic patients. In addition to blocking the synthesis of cholesterol, statins also interfere with the synthesis of lipid intermediates with important biologic effects. In the cholesterol synthetic 993 pathway, intermediate molecules of dimethylallyl pyrophosphate are metabolized by prenyltransferase into geranyl pyrophosphate and subsequently into farnesyl pyrophosphate. These intermediates, geranylgeranyl and farnesyl, participate in protein prenylation, a mechanism by which a lipid moiety attaches covalently to a protein, thereby allowing anchoring into cell membranes and enhancing its biologic activity.
Lester, 59 years: Valvuloplasty is considered a class expandable frame, bovine pericardial leaflets, and a fabric sealing cuff. However, reflex sympathetic stimulation after intravenous verapamil administration may increase the ventricular response over the accessory pathway during atrial fibrillation in patients with Wolff-ParkinsonWhite syndrome, sometimes dangerously so. Zartner P, Toussaint-Goetz N, Wiebe W, Schneider M: Vascular interventions in young patients undergoing transvenous pacemaker revision.
Peer, 27 years: Subendocardial vessels become maximally vasodilated before those in the subepicardium as coronary artery pressure is reduced. The response to a given degree of mitral obstruction may be characterized at one end of the hemodynamic spectrum by a normal cardiac output and high left atrioventricular pressure gradient or, at the opposite end of the spectrum, by a markedly reduced cardiac output and low transvalvular pressure gradient. Pelliccia F, Pasceri V, Marazzi G, et al: A pilot randomized study of ranolazine for reduction of myocardial damage during elective percutaneous coronary intervention.
References