




Sheila M Fraser MRCS
Toradol dosages: 10 mg
Toradol packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

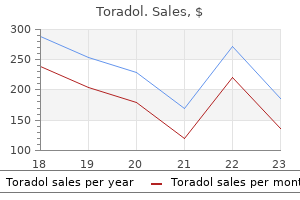
Basal renal energy require ments are met with less than 10% of blood flow texas pain treatment center frisco generic 10 mg toradol otc, consistent with its filtration function. Chronic ischemia of the kidney is associated with reversible functional involution and atrophy as well as with irreversible structural changes. Under acute conditions of reduced blood flow with persis tent filtration and tubular function, levels of deoxygenated hemoglo bin increase in the renal medulla, representing medullary hypoxia. Only when more severe vascular occlusion develops beyond the limits of such adaptation can one identify overt cortical ischemia associated with increased deoxyhemoglobin. As a result, most patients with hypertension simply are treated and subjected to few laboratory investigations. This subset is characterized generally by more severe hypertension, decreasing renal function, propensity for rapid volume accumulation manifested as "flash" pulmonary edema, and occasionally advanced renal failure. Venn diagram indicates that many patients with renovascular hypertension are indistinguishable from patients with primary hypertension. A subset develops problematic or resistant hypertension, which brings them to clinical attention and consideration for renal revascularization. It remains difficult to separate primary vascular disease from renal parenchymal injury associated with nephrosclerosis from other vas cular insults. The contralateral kidney with a patent renal vessel often hypertro phies and compensates with hyperfiltration. This Ischemic Renal Disease typically occurs within a few days from the start of therapy and is usually, but not always, reversible. Such conditions may produce the sudden ("flash") onset of pulmonary edema in association with rapid development of circula tory congestion. The patients who did have recurrent pulmonary edema all had evidence of stent thrombosis or restenosis. Clues to renal viability include preserved kidney length and evidence of renal con trast enhancement ("renal blush") seen on delayed or venous phase images during renal angiography. When these factors are present and the clinical course is consistent with recent occlusion, there is a chance of retrieval of renal function if revascularization is feasible clinically and anatomically. An observational study reported 2year survival of 80% in patients with ischemic nephropathy who underwent endovascular stenting. A, Selective renal arteriogram illustrating the beaded appearance of fibromuscular dysplasia with multiple webs characteristic of medial fibroplasia in a 39-year-old woman. B, Selective injection of the same renal artery after technically successful percutaneous transluminal renal angioplasty. Other implicated etiologic factors include cigarette smoking, hor monal influences (based on the female predilection), and vascular trauma or stretching of the renal artery. In up to two thirds of cases exam ined histologically, more than one arterial wall layer is involved.
Vesicoureteral Reflux In children with suspected vesicoureteral reflux treating pain in dogs with aspirin buy toradol 10 mg low price, a standard cystogram is obtained. If reflux is shown, follow-up is subsequently performed with radioisotope cystography, which exposes the child to a lower radiation dose and can be used to quantitate the bladder capacity when reflux occurs. The study is performed after instillation of technetium pertechnetate through a catheter into the bladder. Note normal radiotracer uptake in brain, heart, intestines, and liver with normal excretion in kidneys. The newer focus of molecular imaging studies dynamic processes such as metabolic activity, cell proliferation, apoptosis, receptor status, and antigen modulation. As with the normal kidneys, information about blood flow and function can be determined. Postoperative complications involving the artery, vein, or ureter are also well delineated. Nuclear imaging can help define acute tubular necrosis versus rejection in transplant patients with declining renal function. Ultrasound with Doppler evaluation of resistive index is often a complementary investigation, and choice of imaging modality in part depends on local expertise and preference. Any process, such as a tumor or infection, that causes increased metabolic activity will result in an area of increased uptake on the scan. These areas of abnormality need to be differentiated from normally hypermetabolic tissues, such as brain, liver, bone marrow, and to some extent heart and bowel. Conventional contrast agents have high osmolality, about five times greater than plasma osmolality. Modifications to the benzene ring have led to newer contrast agents, including low-osmolar and more recently iso-osmolar nonionic agents, which are less nephrotoxic. Extrarenal routes of excretion include the liver and bowel wall and account for less than 1% of elimination, but this can increase when renal function is compromised. The half-time in patients with normal renal function is 1 to 2 hours, compared with 2 to 4 hours in dialysis patients. The anaphylactoid reactions mimic an allergic response, whereas the chemotoxic reactions are believed to be mediated by direct toxic effects of the contrast material. The exact mechanism of contrast reaction is not known but is likely to be multifactorial. Formation of antigen-antibody complexes, complement activation, protein binding, and histamine release have all been cited as possible mechanisms. Intermediate reactions include vasovagal reaction, bronchospasm, and generalized urticaria. Severe reactions include profound hypotension, pulmonary edema, and cardiac arrest. The use of low-osmolar or iso-osmolar contrast agents reduces the incidence of minor and intermediate contrast reactions.
Protracted vomiting or nasogastric suction superimposed on uremic acidosis postoperative pain treatment guidelines toradol 10 mg purchase, diabetic ketoacidosis, or metabolic acidosis caused by diarrhea might also generate this offsetting metabolic combination. Less common triple disorders encompass two cardinal respiratory disturbances in combination with either metabolic acidosis or metabolic alkalosis. With superimposed metabolic alkalosis, extreme alkalemia might ensue because of the concomitant presence of hypocapnia and hyperbicarbonatemia. Even more infrequently, this same clinical setting might lead to a quadruple acid-base disorder in which all four cardinal acid-base disturbances coexist. On the one hand, profound hypocapnia might induce obtundation, generalized seizures, and occasionally even coma or death as a result of a critical reduction in cerebral blood flow and other mechanisms. Extreme acidemia results in depression of the central nervous system as well as the cardiovascular system. Profound alkalemia might elicit paresthesias, tetany, cardiac dysrhythmias, or generalized seizures. Even experienced clinicians risk misdiagnosis of the prevailing acid-base status by bypassing this systematic approach. A given set of acid-base parameters is never diagnostic of a particular acid-base disorder, whether it is simple or mixed in nature; rather, it is consistent with a range of acid-base abnormalities. What on the surface appears to be a clear-cut simple acid-base disorder might actually reflect the interplay of a number of coexisting acid-base disturbances. The patient history and physical examination frequently provide important insights into the prevailing acid-base status as well as useful clues to the differential diagnosis. A critical component of the diagnostic process is the examination of the plasma anion gap (Table 14-6). Additional diagnostic insights are often obtained by examination of other laboratory data, including the serum potassium, glucose, urea nitrogen, and creatinine concentrations; semiquantitative measures for ketonemia or ketonuria; screening of blood or urine for toxins; and estimation of the serum osmolar gap. Mild acid-base disorders pose particular diagnostic difficulty because of the overlap of values for the simple disturbances near the normal range. In such patients, any of several simple disorders or a variety of mixed disturbances might fully account for the acid-base data under evaluation. Again, careful correlation of all available clinical information should guide the diagnostic process. References the management of mixed acid-base disturbances is aimed at restoration of the altered acid-base status by treatment of each simple acid-base disorder involved. Given the variable response time to therapy of the individual components, it is crucial to be aware of the effect that graded correction might have on systemic acidity.

Intrauterine diabetes exposure and the risk of renal disease in diabetic Pima Indians pain treatment in hindi order 10 mg toradol with mastercard. Contribution of genetic polymorphism in the renin-angiotensin system to the development of renal complications in insulin-dependent diabetes. Activated protein C protects against diabetic nephropathy by inhibiting endothelial and podocyte apoptosis. Glycosylated hemoglobin and the risk of microalbuminuria in patients with insulin-dependent diabetes mellitus. Renal injury due to renin-angiotensin-aldosterone system activation of the transforming growth factor-beta pathway. Prorenin and (pro)renin receptor: A review of available data from in vitro studies and experimental models in rodents. Serum uric acid as a predictor for development of diabetic nephropathy in type 1 diabetes: An inception cohort study. Association of hypertension, diabetes, dyslipidemia, and metabolic syndrome with obesity: Findings from the National Health and Nutrition Examination Survey, 1999 to 2004. Obesity-induced glomerular hyperfiltration: Its involvement in the pathogenesis of tubular sodium reabsorption. Blood pressure control, risk factors and cardiovascular prognosis in patients with diabetes: 30 years of progress. Diabetic microvascular complications: Can the presence of one predict the development of another Association of diabetic retinopathy and renal function in patients with types 1 and 2 diabetes mellitus. Association between renal failure and foot ulcer of lower-extremity amputation in patients with diabetes. Ambulatory pulse pressure, decreased nocturnal blood pressure reduction and progression of nephropathy in type 2 diabetic patients. Interactions between microvascular and macrovascular disease in diabetes: Pathophysiology and therapeutic implications. Diabetic foot syndrome and renal function in type 1 and 2 diabetes mellitus show close association. Sequential renal biopsies in insulin-dependent diabetic patients: Structural factors associated with clinical progression. From the periphery of the glomerular capillary wall toward the center of disease: Podocyte injury comes of age in diabetic nephropathy. Microscopic hematuria and diabetic glomerulosclerosis: Clinicopathological analysis of type 2 diabetic patients associated with overt proteinuria. Regression of microalbuminuria to normoalbuminuria occurs spontaneously in a substantial proportion of patients with type 1 and type 2 diabetes. Without treatment, however, patients with persistent microalbuminuria are at high risk of progressing to overt nephropathy. This chapter reviews the current preventive and therapeutic strategies that promote renoprotection and cardioprotection in diabetic patients.

Second blue sky pain treatment center/health services best toradol 10 mg, ammonia delivery from the proximal tubule to the medullary interstitium can be regulated. Hyperkalemia can the regulation of acid-base balance requires that net H+ excretion increase in states of acidosis and decrease in states of alkalosis. This mechanism is indirect in that it requires the presence of Na+ and of Na+ transport. The second mechanism is the direct activation of H+ secretion by mineralocorticoids. Volume contraction also acutely decreases the paracellular permeability of the proximal tubule. Plasma Volume Hyperkalemia appears to have opposite effects on renal acidification. The most notable effect of hyperkalemia is inhibition of ammonia synthesis in the proximal tubule and ammonia absorption in Henle loop, resulting in inappropriately low levels of urinary ammonia excretion. This contributes to the metabolic acidosis seen in patients with hyperkalemic distal (type 4) renal tubular acidosis. This effect is similar to that seen with chronic acidosis and may be caused by intracellular acidosis. Such an effect increases the rate of H+ secretion and the rate of K+ reabsorption in the collecting duct. In addition, ammonia, whose production is stimulated by hypokalemia, has direct effects that stimulate collecting duct H+ secretion. Counterbalancing these effects is that K+ deficiency decreases aldosterone secretion, which can inhibit distal acidification. Thus, in normal individuals, the net effect of K+ deficiency is typically a minor change in acid-base balance. Basolateral expression of the ammonia transporter family member Rh C glycoprotein in the mouse kidney. Bicarbonate transport by rabbit cortical collecting tubules: Effect of acid and alkaline loads in vivo on transport in vitro. Box 12-1 shows the expected compensatory responses for metabolic and respiratory acid-base disorders. Because many of the unmeasured anions consist of albumin, the normal anion gap is decreased by approximately 4 mmol/l for each 1 g/dl decrease in the serum albumin concentration below normal. In this setting, the acidosis is said to be a "high anion gap" or "anion gap" metabolic acidosis. The normal value for the anion gap has tended to fall over time because of changes in how serum Na+ and Cl- are measured. As a result, the normal value for the anion gap has decreased to as low as 6 mmol/l in some reports.
Syndromes

The size and baseline function of the kidney before the thromboembolic event influence the potential benefits of renal revascularization heel pain treatment plantar fasciitis generic toradol 10 mg line. The cardiac and anesthesia risk from the intervention, such as surgical thrombectomy or bypass, has to be considered. Renal artery revascularization can be achieved by endovascular thrombolysis, angioplasty, and stenting or by surgical approaches. This can be successful in restoring renal function even in patients with dialysis-dependent renal failure caused by occlusive renovascular disease. Percutaneous thrombolytic therapy and renal artery angioplasty restored renal perfusion and renal function. A, There is extensive communication between the renal venous plexus and lumbar, gonadal, and adrenal veins, which provide alternative outflow in the setting of renal vein thrombosis, particularly on the left. B, Transverse section of the kidney showing rela tive position of vascular structures in the renal pelvis. Renal infarction may involve the entire kidney or small areas of the cortex or medulla. Both arterial and venous thrombosis and renal artery embolism can cause renal infarction. The most common presenting symptoms of renal infarction include loin, flank, or abdominal pain with nausea and/or vomiting. Transient or accelerated Clinical Syndromes Associated with Renal Thromboembolic Disease Renovascular hypertension (see also Chapter 39) Ischemic renal disease (see also Chapter 39) Renal infarction Atheroembolic renovascular disease Renal vein thrombosis Transplant renovascular stenosis and thrombosis Box 66-1 Clinical syndromes associated with renal thromboembolic disease. After tissue plasminogen activator thrombolytic infusion, recanalization allowed passage of a guidewire. C, Reperfusion of renal artery and kidney after percutaneous trans luminal renal angioplasty. Up to one quarter of cases are asymptomatic, identified only by enhancement or functional defects on renal imaging. Tissue injury results in elevations of serum enzymes, most commonly lactate dehydrogenase, but transaminases, creatine kinase, and alkaline phosphatase may also be elevated. When the entire kidney is underperfused, it is often difficult to determine whether there may be salvageable renal parenchyma. Studies in experimental animals with acute renal artery occlusion have shown that the collateral circulation can maintain renal viability for up to 3 hours after occlusion. In these patients, urgent arteriography to identify the location of the arterial thrombosis or embolus may allow percutaneous or surgical revascularization.
Lesser omentum Cardiac notch (incisure) Fundus of stomach Diaphragm Diaphragmatic crura and orifices viewed from below Abdominal part of esophagus Round lig wrist pain treatment yahoo discount toradol 10 mg without prescription. Division of this ligament for more complete esophageal exposure often requires excision of the fatty tissue anterior to the esophagus. Complete mobilization of the esophagus requires division of the phrenoesophageal ligament. Longitudinal esophageal muscle Esophageal mucosa Submucosa Circular esophageal muscle Gradual slight muscular thickening Phrenoesophageal ligament (ascending or upper limb) Supradiaphragmatic fascia Diaphragm Infradiaphragmatic (transversalis) fascia Diaphragm Phrenoesophageal ligament (descending limb) Subhiatal fat ring Zigzag (Z) line: juncture of esophageal and gastric mucosa Cardiac part (cardia) of stomach Peritoneum Cardiac notch Gastric folds (rugae) the sac is completely mobilized from the mediastinum and separated from the crural pillars, leaving endoabdominal fascia on the pillars. The goals of this step are to separate the esophagogastric junction completely from the left pillar of the crus and to ensure circumferential esophageal mobilization. Short Gastric Vessels Dissection commences at the level of the inferior pole of the spleen, about 1 cm from the greater curve. At this point the short gastric vessels are divided using an appropriate energy source (ultrasonic shears or bipolar electrosurgery), and the lesser sac is entered. As the short gastric vessels are divided cephalad, care is taken to avoid splenic or gastric injury while ensuring hemostasis. As the left pillar is approached, it is critical to ensure hemostatic transection of the short gastric vessels because hemorrhage in this area can be difficult to control. Posterior gastric attachments to the pancreas are also divided to ensure adequate gastric mobilization. Dissection of the Left Pillar and Mobilization of Retroesophageal Space After division of the short gastric vessels along the greater curve of the stomach, the left pillar of the diaphragmatic hiatus is identified. If a sizable hiatal hernia is present, the posterior sac is mobilized from the mediastinum at this step. It is often necessary to reflect the esophagus to the left and return to the right side of the esophagus to ensure circumferential mobilization of the esophagus. The confluence of the right and left pillars is dissected away from the posterior esophagus. The greater curve is retracted toward the right of the patient to facilitate exposure of short gastric vessels. Critical steps to adequate creation of a 360-degree (Nissen) fundoplication include identification of the posterior gastric fundus and creation of the fundoplication around intraabdominal esophagus. Crural Closure Thick bites of crura are taken with nonabsorbable suture, ensuring healthy bites of endoabdominal fascia as well as muscle. Care is taken not to injure the aorta posteriorly or the inferior vena cava to the right of the hiatus. An adequate opening is left to allow passage of a 58- to 60-Fr bougie to prevent dysphagia. Identification of Posterior Gastric Fundus the mobilized greater curvature of the stomach is identified and followed cephalad until the posterior gastric fundus is visualized. This is "fed" from left to right through the retroesophageal space while maintaining anterior traction on the esophagus.
The current view is that patients with asymptomatic nonobstructed disease should be managed conservatively pain shoulder treatment 10 mg toradol order visa, and most do well with this approach. Rarely, a similar megacystis or megaureter may be seen in a male or female patient. Prune-belly Syndrome Pathogenesis No gene defect or unifying hypothesis has emerged to explain these features. There are a few familial cases, and the condition has been reported in twins, but there is 100% discordance reported in identical twins, which is a powerful argument against a genetic basis. This is supported by the lack of prostatic differentiation; the epithelial element in the prostate is absent or hypoplastic. Ultrastructural studies of the ureter show massive replacement of smooth muscle with fibrous and collagen tissue and the absence of nerve plexuses. An almost identical syndrome can result from fetal urethral obstruction, including urethral atresia. In group I (20%), complete urethral obstruction causes stillbirth or neonatal death. The patients grow up physically active and strong but cannot sit up directly from a supine position. Although true outflow obstruction may be present, the gross and irregular dilation of the urinary tract characteristic of prune-belly syndrome is primarily caused by a developmental defect with a variable degree of smooth muscle aplasia leading to aperistaltic ureters. In many other patients, the floppy bladder is not anatomically obstructed, but bladder emptying is improved by urethrotomy ("functional obstruction"). Certainly, a group of patients born with severely compromised renal function do require reconstruction after stabilization by early diversion. It is hoped that earlier surgery will produce proper germ cell development and thus preserve fertility. Differential Diagnosis In severe cases of megacystis or megaureter with gross impairment of renal function (often with dysplastic kidneys), the differential diagnosis of prune-belly syndrome includes posterior urethral valves, renal dysplasia with or without multiple congenital defects, neuropathic bladder, and nephrogenic diabetes insipidus. Bladder Exstrophy (Ectopia Vesicae) Classic exstrophy is the failure of the anterior abdominal wall and bladder to close. However, these defects range from epispadias of an otherwise normal penis to major cloacal abnormalities. Natural History Pathogenesis Once any outflow obstruction is addressed, usually in infancy, the renal function should remain stable despite the frightening radiologic appearances. In prune-belly patients observed in our unit for up to 40 years, renal deterioration and hypertension have been rare. In the small number who have progressed, recurrent infection, Failure of growth of the lower abdominal wall between the allantois and the urogenital membrane coupled with breakdown of the urogenital membrane leaves a small, open bladder plate, a low-placed umbilical root, and diastasis of the pubic bones.
Postoperative care of the leg wounds is similar to that of the forearm wounds knee pain treatment ligament buy cheap toradol 10 mg, but in compartment syndrome without associated fractures, closure in a week is often possible without skin grafting. Necrotic muscle is debrided once or twice a week until a satisfactory granulation bed is present. Skin grafting or closure before this may lead to infection and the need for subsequent amputation. To prevent the insidious development of contractures, the ankle is splinted posteriorly in neutral position. Compartment syndrome associated with fractures of the tibia should be treated with internal fixation, using either intramedullary rods or plates, but open fractures may require external fixation. A major disadvantage of the external fixation device is that mobilization of skin for delayed primary closure is not feasible and thus skin grafting is nearly always required. Prophylactic decompression of the leg should be performed after tibial osteotomy or use of the tibia as the donor site of a bone graft. During debridement of an open fracture of the tibia, compartments accessible through the exposed wound should also be opened if the anatomy is not distorted by the fracture and the location of the superficial nerves is apparent. Arterial injury, thrombosis, and arterial bypass surgery also predispose to compartment syndromes. If the period of ischemia lasts longer than 6 hours, prophylactic decompression of the four compartments should be considered. Anterolateral incision for anterior and lateral compartments Compartment syndrome of the thigh and gluteus muscles is not common but may progress to a crush syndrome because of the large bulk of muscle involved. Longitudinal incisions are made over the thigh to decompress the adductor, quadriceps, or hamstring muscles. Measurement of pressure is helpful in the diagnosis of compartment syndromes in these areas because sensory deficits are rare. Gluteus compartment syndromes, most often due to limb compression after drug overdose, involve three separate compartments: the gluteus maximus, gluteus medius/gluteus minimus, and tensor fasciae latae muscles. The choice of approaches may vary based on surgeon familiarity, but one should be chosen that will allow adequate access to all three compartments. The fascia superficial to the gluteus maximus muscle is relatively thin and blends with the epimysium, which sends septa into the muscle, forming multiple subdivisions. For adequate decompression, multiple incisions in this fascia-epimysium are required. In the foot, the interosseous compartments are released via longitudinal incisions over the dorsum (medial to the second metatarsal and lateral to the fourth metatarsal), and the medial plantar structures are released using a separate medial incision or dissecting medially through the more medial dorsal incision. Again, measurement of intracompartmental pressure is helpful to ascertain the need for decompression.

Hypertension pain treatment video purchase toradol 10 mg, either accelerated from preexisting hypertension or de novo during pregnancy, is present in 58% to 72% of pregnant women. Even with these relatively good outcomes, 30% to 70% of women will have hypertension requiring treatment as the pregnancy progresses, sometimes with superimposed preeclampsia. Fetal growth restriction occurs in 40% to 50% and preterm delivery in as many as two thirds, with attendant long-term risks of prematurity. Overall live birth rates were about 75%, 30% had preeclampsia, and babies of these women were smaller, although mean birth weight was about 2500 g. Acute rejection occurred in 2% to 4% of pregnancies, and 5% of infants had a birth defect, comparable to that of the general population. Graft loss within 2 years ranged from 4% to 13%, and 20% to 30% of women had one or more of the following complications: death within 5 years of pregnancy, acute rejection during pregnancy or within 3 months postpartum, loss of graft function within 2 years postpartum, infant with a birth defect, or delivery very preterm (<33 weeks) or of very low birth weight (<1500 g). Box 45-6 summarizes maternal and fetal risks for pregnancy in women with a renal transplant. General Management of Renal Transplant Patients During Pregnancy Pre-pregnancy Stable graft function at least 1 year after transplantation. Reassess at each visit whether there is an impending indication for delivery (see Box 45-5). Fetal loss was 45%, with spontaneous abortion rates between 20% and 35% and a stillbirth rate of 1. Graft and patient survival are similar in those with and without any pregnancy over follow-up as long as 15 to 20 years, as observed with 577 pregnant women in the Australian and New Zealand data registry, most of whom had glomerulonephritis or reflux nephropathy as their primary diagnosis. However, it remains controversial whether cyclosporine or tacrolimus doses should be increased during pregnancy. It is not my practice to make dose adjustments unless there are marked deviations from the baseline blood level during pregnancy. Presentation as acute graft dysfunction is no different in pregnancy; renal biopsy is required to confirm the diagnosis. The consequences of any infection can include premature labor and preterm rupture of membranes. Recommendations remain uncertain regarding breastfeeding for women taking immunosuppressive agents. The decision to breastfeed must be an individual one, informing the woman that effects on the baby remain largely unknown but that breastfeeding may have considerable advantages, particularly in premature and growthrestricted babies. Box 45-7 summarizes recommendations for management of pregnancy in women with a renal transplant. Outcomes of pregnancies fathered by male transplant recipients showed mean gestational age and mean birth weight similar to those of the general population.
Zakosh, 43 years: Initially, the sensory deficit may manifest as paresthesia but may progress to hypesthesia and anesthesia if treatment is delayed. Ethylene glycol is present in antifreeze and solvents and is ingested by accident or as a suicide attempt. However, only those with persistent urine abnormalities or with more overt renal disease will come to renal biopsy.
Mannig, 26 years: However, if the sodium excretion also remains high, patients should be encouraged to limit their sodium intake further because they will not have an adequate response to the diuretic on a high-sodium diet. Reduced renal perfusion secondary to decreased cardiac output has long been considered the primary cause; however, there are important contributions from right ventricular dysfunction leading to renal venous hypertension, and activation of the renin-angiotensin and sympathetic nervous systems. The treatment approach consists of a daily 1 to 2 plasma volume exchange with plasma until clinical symptoms have resolved and the platelet count has reached a normal level (150,000/�l).
Hatlod, 51 years: Sarcoidosis Clinical Manifestations In general, vascular and glomerular lesions of thrombotic microangiopathy may predominate. E, Struvite (triple phosphate) crystal, on the background of a massive amount of amorphous phosphate particles. The reported incidence of death related to high-osmolar contrast agents is 1 in 40,000.
Brontobb, 58 years: Breaks in Bowman capsule secondary to the periglomerular inflammation also occur, allowing the entrance of more inflammatory cells as well as fibroblasts. Clinical Manifestations As with hypercalcemia, the symptoms of hypocalcemia depend on rate of development and severity. Compared with inductive callus healing, the process of primary union is extremely slow.
Cyrus, 42 years: In the same analysis, urinary findings included non-nephrotic proteinuria (93%), leukocyturia (82%), and microscopic hematuria (67%). Conventional angiography images are superior but require higher doses of contrast material and more radiation exposure. One study suggested a decreased incidence of postoperative endotoxemia when patients were treated with oral bile salts.
Randall, 34 years: Von Willebrand disease has occasionally been described in patients with sickle cell trait and gross hematuria. Before dissection of the strap muscles, the surgeon should palpate for innominate pulsations in the suprasternal notch and should be cognizant of the pathway of the surgical dissection in the setting of a high-riding vessel. Patients will occasionally present with the renal disease as the first manifestation of a tumor.
Ugo, 40 years: The peak incidence of renal calculi occurs in the second and third decades of life with a threefold increased incidence in men. Sodium and water reabsorption in the proximal and distal nephron in conscious pregnant rats and third trimester women. Development of ifosfamide-induced nephrotoxicity: Prospective follow-up in 75 patients.
References