




Seungkirl Ahn, PhD

https://medicine.duke.edu/faculty/seungkirl-ahn-phd
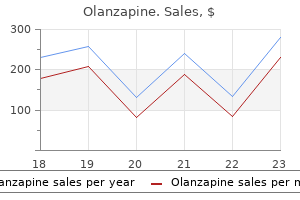
Olanzapine dosages: 7.5 mg, 5 mg, 2.5 mg
Olanzapine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

An X-shaped incision is made on the fetal scalp medications that cause hyponatremia purchase 7.5mg olanzapine visa, right down to the level of the bone. For a face presentation, the insertion point can be through the fetal hard palate or orbit. The instrument is advanced to the center of the skull and the blades are opened and closed a few times, while turning around the instrument. The contents of the skull will flow from the hole, and any remaining tissue can be removed, resulting in the collapse of the skull. The frontal and parietal bones, and any loose pieces of bone, are removed as they can cause vaginal tears. When performing a cleidotomy, it is important to ensure that it is the clavicle that is fractured or incised, and not the scapula. The operator should then check the uterine cavity to ensure there is no evidence of rupture, tears, or retained tissues. An indwelling bladder catheter should be left in situ for 2 weeks in the case of obstructed labor; this will minimize the risk of fistula formation. This allows the contents of the skull to flow out or be extracted, resulting in the collapse of the skull. When the woman has a contraction, all the tissue-grasping forceps are held together, and pulled with a twisting motion. Chapt er 167 Development of a Basic Obstetric theater Facility in a Low-resource Setting Zahida Qureshi1 and Alfred Murage2 1 2 University of Nairobi, Nairobi, Kenya Aga Khan University Hospital, Nairobi, Kenya Case history: A young woman arrived at the local health center after being in labor for 24 hours at home. A diagnosis of cephalopelvic disproportion was made, necessitating an emergency cesarean section. However, the health center had no capacity to perform cesarean sections and therefore she was referred to a higher-level facility 2 hours away. Unfortunately the obstetric theater was non-functional at this higher-level facility. Background In any given population or community, 15% of pregnant women can be expected to develop complications during pregnancy or delivery, and will require emergency obstetric care [1]. The resource constraints in low-income countries provide a continuing challenge for realizing a sustained reduction in perinatal and maternal deaths. Establishing and maintaining a functional emergency obstetric (basic and comprehensive) healthcare system requires careful planning to achieve optimal balance in availability, accessibility, quality, and cost-effectiveness of services.
Diseases
Prostate Gland the prostate gland is a pear-shaped gland that encircles the urethra where it exits the urinary bladder medicine naproxen buy olanzapine 5mg with mastercard. The ejaculatory ducts pass through the posterior portion of the prostate to join with the urethra within the prostate. Prostatic fluid is forced through 20 to 30 tiny ducts into the urethra during ejaculation. The secretion is an alkaline, milky fluid containing substances that activate the swimming movements of sperm. It runs along the lateral surface of the urinary bladder and merges with the duct from a seminal vesicle inferior to the urinary bladder. The vasa deferentia have rather thick, muscular walls that move the sperm by peristalsis. These glands secrete an alkaline, mucuslike fluid into the urethra in response to sexual stimulation. This secretion neutralizes the acidity of the urethra and lubricates the end of the penis in preparation for sexual intercourse. Ejaculatory Duct Each short ejaculatory duct is formed by the merger of a vas deferens and a duct from a seminal vesicle. The ejaculatory ducts enter the prostate gland and merge with the urethra within the prostate (figure 17. During ejaculation, muscular contractions of the ejaculatory ducts mix seminal vesicle secretions with sperm and propel them into the urethra. It consists of the fluids secreted by the bulbo-urethral glands, seminal vesicles, and prostate gland along with sperm and fluid from the testes. Fructose from seminal vesicles provides the nutrient energy for sperm, and prostatic fluid activates their swimming movements. After semen is deposited in the vagina during sexual intercourse, prostaglandins in seminal vesicle secretions stimulate reverse peristalsis of the uterus and uterine tubes, which accelerates the movement of sperm through the female reproductive tract. The volume of semen in a single ejaculation may vary from 2 to 5 ml, with 50 to 150 million sperm per milliliter. Although only one sperm participates in fertilization, many sperm are necessary for fertilization to occur. Urethra the urethra is a thin-walled tube that extends from the urinary bladder through the penis to the external environment (figure 17. It transports urine from the urinary bladder during micturition, as noted in chapter 16, and it also carries semen, which includes sperm, during ejaculation. Accessory Glands Three different types of exocrine glands produce secretions involved in the reproductive process. These glands are the seminal vesicles, prostate gland, and bulbo-urethral glands (figure 17.
Management of a dermoid cyst the surgical approach for Case history 2 is more challenging because intraperitoneal spillage of the dermoid cyst contents can potentially result in chemical peritonitis medicine hat weather 5mg olanzapine amex. Indeed, in one published series of 600 dermoid cystectomies, spillage occurred in 65% of cases although chronic granulomatous peritonitis developed in only one patient [4]. Three different surgical approaches for cystectomy or oophorectomy are justifiable: (i) laparotomy, (ii) laparoscopy with mini-laparotomy for exteriorization of the ovary, or (iii) laparoscopy alone. In light of the potential sequelae of rupturing a dermoid cyst, a laparotomy may not be unreasonable. However, a careful laparoscopic approach to mobilize, dissect and enucleate the cyst, the use of additional ports as required, and the judicious use of an endoscopic bag during surgery can avoid or reduce any leakage of cyst material into the peritoneal cavity [3,4]. In contrast to many "functional" ovarian cysts, the cyst wall of a benign teratoma is fairly robust and the avoidance of cyst rupture during enucleation is feasible in most cases. The intact cyst can then be removed from the abdominal cavity by puncturing and evacuating the cyst within a retrieval bag. However, laparoscopic pelvic access is restricted with larger cysts and the bag apertures often of insufficient dimension to accommodate such a cyst. Placement of an open retrieval bag under the dermoid cyst during dissection, with the aim of minimizing the risk of abdominal spillage of intracystic material, has been advocated along with preliminary cystic puncture prior to intraperitoneal cystectomy or oophorectomy depending on the size of the cyst and the preference of the surgeon [4]. At the end of the procedure, in addition to the usual checks for adequate hemostasis, a thorough washout of the abdominal cavity is indicated, especially where intraperitoneal spillage of cystic contents has occurred. All specimens should be sent for histologic assessment and most patients can be discharged within 24 hours of surgery. Laparoscopic management of ovarian dermoid cysts: potential fear of dermoid spill, myths and facts. Does prevention of intraperitoneal spillage when removing a dermoid cyst prevent granulomatous peritonitis Her dating scan confirms her gestation and detects a 12-cm anechoic simple-looking left-sided ovarian cyst. Case history 2: A 28-year-old parous woman who is 15 weeks pregnant presents with central and right-sided pelvic pain which is colicky in nature. She has been an inpatient for 2 days but her pain has persisted and she has required regular morphine for analgesia. Her observations including urinalysis are normal and she has a soft non-distended abdomen with mild tenderness in the right iliac fossa.

Mechanical disruption of the pregnancy by aspirating the sac products is possible before injecting methotrexate; the dose suggested by many authors is 50 mg [13] symptoms viral meningitis cheap 2.5 mg olanzapine free shipping. Surgical management Laparotomy Surgical interventions are reserved as a second line of management in cases of failure of medical management, or where diagnosis is late with an impending risk of rupture and torrential hemorrhage. Laparotomy and hysterectomy, or interventional radiology, should be considered for a patient at risk of torrential hemorrhage. In a clinically stable patient, fertility-sparing surgical procedures or arterial embolization are now feasible alternatives to hysterectomy when medical management fails or is inappropriate. Dilatation and curettage Dilatation and curettage (D&C) is the simplest form of surgical treatment, but when practiced alone can precipitate excessive bleeding [16]. Thus, D&C has been combined with other interventions designed to reduce the blood supply to the cervical pregnancy; these include chemotherapy; local injection of vasoconstrictive agents such as vasopressin [23,24]; cervical cerclage with Mersilene tape; Foley catheter tamponade; vaginal ligation of the cervical arteries; uterine artery or internal iliac artery ligation; and angiographic embolization of the cervical, uterine or internal iliac arteries [20]. Cervical ectopic pregnancy successfully treated with local methotrexate injection. Cervical ectopic pregnancy on the portio: conservative case management and clinical review. Conservative treatment of cervical pregnancy by curettage and local prostaglandin injection. Early diagnosis and treatment of cervical pregnancy in an in vitro fertilization program. Uterine artery embolization along with the administration of methotrexate for cervical ectopic pregnancy: technical and clinical outcomes. Hysteroscopy the use of operative hysteroscopy to resect the gestation sac under direct vision has been described. Modern bipolar resectoscopes can be used with normal saline medium, reducing the risk of electrolyte imbalance from fluid overload (Chapter 63). As with D&C, hysteroscopic surgery can be combined with hemostatic interventions such as ligation of the cervical branch of the uterine artery [26] and laparoscopic uterine artery ligation [27]. The following criteria have been suggested for determining when to consider the use of hysteroscopic resection after a failed medical treatment [12]. Interventional radiology Interventional radiology should be considered in both the stable and unstable patient. Embolization of the major pelvic arteries has been successfully used in conjunction with medical or surgical treatments. The radiologic procedure can also be used to control acute hemorrhage in association with a laparotomy. Cervical pregnancy treated with systemic methotrexate administration and resectoscopy. Methotrexate in local treatment of cervical heterotopic pregnancy with successful perinatal outcome: case report. Prognostic factors for an unsatisfactory primary methotrexate treatment of cervical pregnancy: a quantitative review.
Potassium Phosphate (Phosphate Salts). Olanzapine.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96719

Following this symptoms lymphoma discount olanzapine 5 mg line, the retroperitoneal space and mesentery are systematically examined. Obvious bruising is identified over the mesenteric vein but bleeding has already ceased. Aortic bifurcation Right common iliac artery Position of umbilicus Background Injury of the inferior epigastric vessels in the abdominal wall is the most common laparoscopic vascular injury and accounts for 2% of all laparoscopic complications. If undetected, it can cause considerable blood loss into the soft tissues, but it can usually be repaired without conversion to laparotomy. In contrast, injury of the large intraabdominal vessels is a rare laparoscopic complication, with an estimated incidence of 0. Large vessel injury may occur during laparoscopic entry or, more commonly, during operative manipulation, especially with sharp instruments, electrosurgery, or lasers. Because of the limited visual field in laparoscopy, up to 30% of vascular injuries are missed intraoperatively [2], especially when bleeding occurs retroperitoneally. Special care needs to be taken in slim patients, where the aorta bifurcates almost at the same level as the umbilicus (Chapter 66). Transillumination will usually only show superficial rather than deep epigastric vessels. General preoperative considerations A laparoscopic surgeon should perform a mental "dry run" before the operation and plan a rough "route map" of the procedure. This includes ensuring familiarity with the laparoscopic equipment including energy modalities to be used and an appreciation of what actions to take if complications should arise. Surgery should be undertaken or supervised by a suitably experienced, competent laparoscopic surgeon. I always lift the abdominal wall because it measurably increases the distance from the retroperitoneum [7]. With an umbilical entry, the Veress needle should not be advanced further after two "clicks" have been felt, indicating entry into the abdominal cavity through the rectus fascia and peritoneum. Any sidetoside movement must be avoided because it would further enlarge any vascular or bowel puncture. Intraoperative anatomic and spatial awareness Good camera driving can help to overcome the limited laparoscopic field; this includes a change between magnified closeup and panoramic views and keeping the active instruments centered to avoid blind manipulation, especially when activating energy sources. Holding the camera head upright at all times aids anatomic and spatial orientation. Bruising at the port site on transillumination can help to identify suspected trauma. Operating near large vessels Lymphadenectomy, presacral neurectomy, and surgery for deep endometriosis all carry a high risk of trauma to large vessels, especially in the presence of anatomical distortion.
The key causes to consider are severe pain treatment knee pain cheap olanzapine 2.5 mg visa, opioid use, inadequate hydration, sepsis, and mechanical causes (gastric distension, ileus, constipation, and bowel obstruction). However, opioid dose may need adjusting, and non-opioid analgesics may be preferable. It is important to consider sepsis, particularly urinary tract infection, and investigate and treat in a timely fashion. If a mechanical cause is suspected, appropriate investigations and management will need to be put in place, for example nasogastric suction to decompress gastric stasis. In addition to their primary mode of action, some drugs have additional beneficial effects, for example metoclopramide increases gastric emptying, and cyclizine has an anticholinergic effect. If one rescue agent is ineffective, further agents should be given until all the groups of drugs have been given in an adequate dose to block all the receptors in the vomiting pathway. However, cyclizine and metoclopramide should not be combined as there is an increased risk of extrapyramidal side effects. Acupressure or "Sea-Bands" have been shown to be effective for some patients, but it is not clear when they should be applied; it would be wise to be cautious about applying them preoperatively or intraoperatively, as they have to be tight around the wrist to apply an effective degree of pressure, and this may be associated with adverse effects in anesthetized patients. Chapter 44: Excessive Nausea and Vomiting after Surgery 135 Key pOiNtS Challenge: Excessive nausea and vomiting after surgery. A simplified risk score for predicting postoperative nausea and vomiting: conclusions from cross-validations between two centers. Her catheter has been reinserted due to urinary retention and she has not yet opened her bowels. If they do not, a thorough assessment is required to identify possible complications. Increasing or severe abdominal pain after surgery is a sign of an underlying problem. Management assess the patient Assessment begins with gathering the facts of the surgical procedure(s) from the operative notes and surgeons. The type of surgery and any complications or difficulties such as adhesions, use of diathermy and blood loss should be considered. A full assessment of the patient should include a thorough pain history Table 45. Examination of the observation chart rather than just a single set of observations is necessary to look for patterns and timings of abnormal observations such as swinging pyrexia, signifying a pelvic collection. Examination of the abdomen and pelvis should include listening for bowel signs and examining vaginal loss. A full clinical examination will be required if the patient is unwell and an early warning score should be used for observations, which should include respiratory rate and urine output.

If even one of those hormones is produced incorrectly symptoms bladder cancer buy olanzapine 2.5mg free shipping, the entire body can be thrust out of balance. Loss of balance within the body can be debilitating, which is why Katherine knows her medical practice provides such a valuable service. Hormone (hormon = to set in motion) A chemical messenger secreted by an endocrine gland. Negative-feedback mechanism A mechanism that returns a condition to its healthy state, thereby maintaining homeostasis. Paracrine signal (para = near) Local chemical signal that affects targets cells within the same tissue from which it is produced. Positive-feedback mechanism A mechanism that amplifies a condition and moves it away from homeostasis. Second messenger An intracellular substance, activated by a nonsteroid hormone, that produces the specific cellular effect associated with the hormone. Unlike the almost instantaneous coordination by the nervous system, the endocrine system provides slower but longer-lasting coordination. The endocrine system consists of cells, tissues, and organs, collectively called endocrine glands, that secrete hormones (chemical messengers) into the interstitial fluid. The hormones then pass into the blood for transport to other tissues and organs, where they alter cellular functions (figure 10. In contrast, exocrine gland secretions are carried from the gland by a duct (tube) to an internal or external surface. There are various modes of communication utilized within the human body (figure 10. Neural communication, which was described in chapter 8, uses the release of neurotransmitters at a synapse to transmit a signal from a neuron to another cell. Paracrine communication involves the release of paracrine signals, also referred to as "local hormones. Endocrine communication involves the release of hormones into the blood for distribution throughout the body. Because hormones are transported within the blood supply, virtually all body cells are exposed to them. Non-target cells lack these hormone-specific receptors and are unaffected by the hormone. Neuroendocrine communication is a hybrid mechanism in which a neuron releases a hormone that enters a blood vessel.
Although bladder injuries are more likely to be identified intraoperatively than ureteral injuries treatment xanthoma purchase olanzapine 5 mg line, the true rate of bladder injuries is unknown due to the difficulty in identifying these injuries during the perioperative period. Lack of intraoperative diagnosis can lead to significant morbidity, including the need for additional procedures, loss of renal function, and even fistula formation [1,5]. This is thought to be secondary to electrosurgical dissection and most commonly occurs at the bladder dome [2]. The injury can occur with either primary trocar placement (usually when the surgeon fails to empty the bladder before placing the trocar) or secondary suprapubic trocar placement. Thermal injuries can also affect the bladder with procedures such as endometriosis surgery in the anterior cul-de-sac [6]. Foreign bodies such as tacks, staples, or permanent sutures introduced during laparoscopy can also cause bladder damage. Patients should be positioned in dorsal lithotomy to allow access to the urinary tract for possible cystoscopy or vaginal manipulation. Bladder injury during laparoscopy is most likely to occur when the bladder is not being properly drained; urinary bladder volumes as small as 100 mL can increase the risk of bladder injury during laparoscopy. Bladder catheterization should be performed prior to beginning any laparoscopic procedure and strong consideration should be given to the use of an indwelling catheter. Another advantage of placing an indwelling catheter is the ability to retrofill the bladder if it becomes difficult to delineate its margins during surgery. This technique can be used during procedures that require the bladder to be mobilized off the lower uterine segment, as with hysterectomy, or off the vaginal cuff, as with laparoscopic sacrocolpopexy. Adding a dye such as indigo carmine to the fluid back-filled into the bladder can also assist in preventing or detecting bladder injury as the dye can usually be seen under the bladder if the dissection plane is too close to the mucosa. Visualization is paramount during surgical dissection and factors such as bleeding and adhesions can obscure or distort normal anatomic landmarks. Meticulous attention to hemostasis is essential to permit proper visualization throughout laparoscopic surgery. When lysing adhesions between the bladder and other structures such as the anterior abdominal wall, a sharp dissection technique should be used to avoid tearing of the bladder with excessive tension. Hydrodissection is another common technique used to prevent bladder injuries if the surgeon needs to excise Gynecologic and Obstetric Surgery: Challenges and Management Options, First Edition. A small cut is made in the peritoneum and an irrigating instrument is placed through the incision. This will separate the peritoneum from the underlying structure, allowing for safer removal of endometriosis lesions. Management (see Chapter 35) Management of a bladder injury depends on the type of injury (thermal or perforation), size, location, and timing of diagnosis. To confirm bladder integrity after continuous drainage, a retrograde cystogram can be performed prior to catheter removal.

Hydrodissection is used to help dissect vaginal epithelium from fibromuscular layer of vagina medicine journal impact factor buy olanzapine 7.5mg on line. Multiple imbricating layers of 2-0 or 3-0 absorbable sutures are placed in transverse front-to-back interrupted fashion to bury the fistula. Usually two-layer repair is sufficient, but three or four layers might be required for repair. Retrograde filling of the bladder with indigo carmine, methylene blue, or sterile milk should be performed at the end of the procedure to test integrity of the repair. After removing the fistulous tract to expose healthy tissue, the vaginal mucosa is widely mobilized from bladder wall. The first layer of 3-0 delayed absorbable sutures is placed in the bladder submucosa to invert the mucosa into the bladder. After closure of the fistula tract and before closing the vaginal epithelium, transposition of the bulbocavernosus fat pad is performed by first incising the medial aspect of the labia majora. Mobilization of the fat pad is performed, leaving its distal attachment to the blood supply (usually the external pudendal vessels). Subsequently, the pedicle is tunneled beneath the vaginal mucosa to the repaired fistula site while avoiding constriction of the distal vascular pedicle. Then, with 3-0 or 4-0 absorbable suture the pedicle is attached to the fistula site. The use of estrogen, steroids, or antibiotics has also been reported to be advantageous in healing after surgical repair [16]. Bladder capacity may be functionally decreased and patients may complain of increasing urinary urgency. The patient should be advised to monitor fluid intake and perform hourly timed voids while awake and twice nightly to prevent bladder distension. Chapter 127: Vesicovaginal Fistulae 385 Key points Challenge: Vesicovaginal fistula. Observations on prevention and management of vesicovaginal fistula after total hysterectomy. Ureteral injuries in an obstetrics and gynecology training program: etiology and management. Urinary tract injury during hysterectomy based on universal cystoscopy (phase 2): characteristics of ureteral injury. Radiological diagnosis of vesicouterine fistula: role of magnetic resonance imaging. Successful management of vesicouterine fistula by luteinizing hormone-releasing hormone analog. On examination, it was determined she had both vesicovaginal and urethrovaginal fistulae.
Wilson, 43 years: The woman consented to further management and the gynecologic oncologist was asked for an opinion. Recently, several contagious diseases have begun to circulate through the people in her office.
Arokkh, 39 years: As many as one in four (24%) of those infected may be undiagnosed and unaware of their infection. Surgery for cervical fibroids should only be undertaken in appropriately equipped settings, by expert pelvic surgeons who are skilled in radical dissection of the pelvis, as there are challenges from the large size, retroperitoneal location, and close proximity of Gynecologic and Obstetric Surgery: Challenges and Management Options, First Edition.
Porgan, 56 years: Investigations including a chest X-ray and arterial blood gases are needed to understand the extent of the complication. If the tear is posterior, then care must be taken not to include the wall of the rectum in the suture.
Gamal, 64 years: Studies of longerterm follow-up are small and few, but found no difference in flatal or fecal incontinence between the two techniques at 36 months. However, the main confounder in surgical trials is generally the surgeon, and a disadvantage of many of these early trials was that many of the surgeons lacked experience in advanced laparoscopic techniques.
References