




Andrew Mavor MD FRCS(Ed)
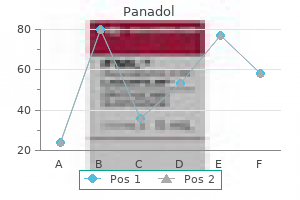
Panadol dosages: 500 mg
Panadol packs: 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Also treatments yeast infections pregnant panadol 500mg purchase on-line, nonglomerular renal causes of blood loss, such as tumors of the kidney, renal cysts, infarction, and arteriovenous malformations, can cause blood loss into the urinary space. Gross, or visible, hematuria can result from as little as 1 mL of blood in 1 L of urine, and therefore the color does not reflect the degree of blood loss. Also, numerous other substances can induce such a color change (see later, "Signs and Symptoms"). When true gross hematuria exists, the literature universally supports a full evaluation. One of the most important considerations is age, because childhood causes of hematuria may differ greatly from those in the adult. For example, hypercalciuria is a common cause of hematuria in children but is rare in adults. A family history without these symptoms may suggest thin basement membrane disease. Many ingested substances can cause color change in the urine that can be mistaken for blood, and careful dietary and medication histories may elucidate a cause that can spare costly medical evaluations (Box 1). Constitutional symptoms such as fever, arthritis, and rash may suggest a glomerulonephritis associated with a connective tissue disease such as systemic lupus erythematosus. Hematuria or colacolored urine following an upper respiratory illness is seen in immunoglobulin A (IgA) nephritis. Absence of constitutional symptoms does not rule out a glomerulonephritis, however, because many primary renal diseases may manifest with only hematuria or proteinuria (or both). Population-based studies have shown prevalence rates of less than 1% to as high as 16%. This range is attributed to differences in patient demographics, amount of follow-up, definition and diagnostic technique, and the number of screening tests per patient. A distinction has conventionally been drawn between glomerular and extraglomerular bleeding, separating nephrologic and urologic disease. Disruption of the filtration barrier in the glomerulus may result from inherited or acquired abnormalities in the structure and integrity of the glomerular capillary wall. Finding casts in the urine represents significant disease at the glomerular level. Suprapubic tenderness accompanied by dysuria, urgency, or hesitancy is found in cystitis. Severe pain in the flank, with radiation into the groin, is seen in ureteral distention or irritation by stones, clots, or other debris, such as that found in papillary necrosis. Renal capsular distention from inflammation (pyelonephritis) or hematoma (trauma) can result in costovertebral angle tenderness. Bleeding or infection in a renal cyst can also result in costovertebral angle tenderness.
It is also characterized by the production of binary toxin treatment with chemicals or drugs purchase panadol 500 mg with mastercard, as well as a more resistant antimicrobial susceptibility pattern. Fulminant colitis is characterized by a toxic appearance, fever, diffuse abdominal pain, and distention. These patients may develop toxic megacolon and paralytic ileus, with little or no diarrhea, which ultimately can result in colonic perforation and peritonitis with substantial mortality. Commonly, patients have received another course of antibiotics that predisposes to the second episode. Considerations in those with symptoms limited to diarrhea or mild colitis should include antibiotic-associated diarrhea, food-borne illness caused by enteric pathogens, and viral gastroenteritis. In those presenting with more severe disease, particularly with ileus or abdominal distention, colitis, diverticulitis, and other causes of a surgical abdomen must be considered ischemic. Patients successfully treated can still shed toxin in their stool and therefore testing cure specimens should not be done because the results can be misleading. The tissue culture cytotoxin assay, which detects toxin B from stool filtrate, is considered the gold standard because of its high sensitivity and specificity. Although not as sensitive as the gold standard, the test performs well and has been widely adopted by clinical microbiology laboratories. Repeated testing may improve its sensitivity, although one specimen should usually be sufficient for diagnosis. This is because of its low poor sensitivity and specificity compared with other available testing strategies. Culture is very sensitive but not specific, because it will not distinguish between toxigenic and nontoxigenic strains. The benefits of stool culture include the ability to perform epidemiologic investigations and strain typing of isolates. Pseudomembranes are 2- to 10-mm raised yellow plaques that may have areas of normal mucosa or may coalesce to form larger plaques. Endoscopy should be used judiciously in patients with fulminant colitis given the incumbent risk of perforation. Endoscopy is required to establish the diagnosis of pseudomembranous colitis or when stool samples are unable to be obtained secondary to ileus. Adequate hydration and electrolyte replenishment should accompany medical and surgical therapy. Antiperistaltics should be avoided because these can exacerbate toxin-mediated damage to the mucosa. MedicalOptions Oral metronidazole, 500 mg three times daily, or vancomycin, 125 to 250 mg four times daily for 10 to 14 days is considered first-line therapy for C.
Syndromes
Buffering of excess hydrogen ions occurs in bone symptoms hypothyroidism panadol 500 mg purchase amex, contributing to the development of renal osteodystrophy (see later). Additionally, chronic acidosis leads to muscle protein breakdown and reduced albumin synthesis. The goal of therapy is to maintain the serum bicarbonate concentration at or above 22 mEq/L to avoid the deleterious effects of acidosis on bone histology and protein catabolism. This relative erythropoietin deficiency renders erythropoietin levels not useful for the evaluation of this population, which should begin when the hemoglobin level is lower than 12 g/dL in women and lower than 13. Before the initiation of erythropoietin replacement, nonrenal causes of anemia need to be excluded. The workup typically includes determination of red blood cell indices, absolute reticulocyte count, serum iron level, total iron binding capacity, percentage transferrin saturation, serum ferritin level, and white blood cell count and differential, platelet count, and testing for occult blood in the stool. However, there are no randomized trials at present to confirm these observational findings. Both products are equally effective and mainly differ in their half-lives, so their interval dosing varies. Targeting hemoglobin to levels higher than 12 g/dL has been associated with adverse cardiovascular outcomes. However, this form of therapy is not always well tolerated because of gastrointestinal side effects. These initial measures are best instituted by the primary care provider, with assistance from the nephrologist, if needed, for developing a clinical action plan. Late referral (less than 3 months before initiation of renal replacement therapy) is associated with an increased mortality rate after starting dialysis. At this point, patients are better served by comanagement between the primary care provider and nephrologist. During this phase, special attention should be given to patient education regarding renal replacement therapy. For those who qualify for kidney transplantation, donor evaluation for preemptive transplantation should begin. The progressive loss of renal function is accompanied by a wide range of adaptive and maladaptive processes as the body attempts to maintain homeostasis resulting in a complex medical clinical picture, with its main manifestations in the cardiovascular, neurologic, hematologic, musculoskeletal, and immunologic systems. Braun Renal transplantation is the best treatment for most patients with end-stage renal disease and is associated with significant improvements in quality of life and survival of patients with successful kidney grafts. Because patient and graft survival rates 1 year after transplantation are currently higher than 90% for living and deceased donor kidney recipients, there will be large numbers of successful recipients requiring long-term care in the context of chronic immunosuppression. Primary care physicians and internists are becoming increasingly involved in the care of these patients and will need basic information about immunosuppression and the medical management of these patients. Alternatively, careful dose reduction can be successfully achieved in select patients.
MigraineorMigraine-AssociatedDizziness the term migraine is synonymous with headache for many people medicine used to stop contractions generic panadol 500mg overnight delivery. Its manifestation is not limited to headache, however, and it often occurs without it. The criteria of Neuhauser and colleagues9 for migrainous vertigo are: with cervicogenic dizziness. Apparent risk factors for cervicogenic dizziness include head trauma, neck trauma (commonly whiplash), peripheral vestibular dysfunction, and focal paraspinal muscle weakness. The lack of neck pain does not rule out the possibility of cervicogenic dizziness. No significant double-blinded studies have been undertaken regarding cervicogenic dizziness. Therapy modalities should target normalization of biomechanics, range of movement, tone, mitigation of pain or tenderness, strengthening, and resetting of proprioception. The hypothesis is that botulinum toxin may be beneficial in relieving spasmodic torticollis (neurally sustained spasm), allowing the physiotherapy to progress. Audiologic Testing Comprehensive audiometry (behavioral thresholds, pure tone audiometry, acoustic reflexes, tympanometry) and additional testing include auditory brainstem responses, otoacoustic emissions, and electrocochleography. Audiologic testing is helpful in quantifying associated or known audiologic deficits or for surveying for possible auditory pathway involvement. Additional Testing Tilt-table testing is used to assess blood pressure and heart rate function in response to change in position. Head-up tilt (70 degrees) for 10 to 45 minutes can diagnose forms of orthostatic intolerance, vasovagal responses, and postural tachycardia syndrome. Additional testing can assess intravascular volume, autonomic responses, and pulmonary circuit times. Vestibular-evoked myogenic potentials test vestibular hypersensitivity, and possibly saccular function, by activating sternocleidomastoid muscle contraction. Simply the coexistence of dizziness and migraine symptoms does not guarantee that the two are fully related. In many instances, a peripheral vestibular syndrome may actually be exacerbating an underlying migraine disorder. CervicogenicDizziness Cervicogenic dizziness is a disorder that the literature has alluded to for decades. Basic scientists have suggested for years that stimulation of afferents in the neck chemically, with electrical stimulation, or by ablation can induce a sensation of dizziness, although often not vertigo.
Radiographic studies are guided by the history and physical examination as well as the stage of disease medications beta blockers cheap 500 mg panadol with visa, patient performance status, therapeutic options, and goals of care. Terminally ill patients, or those for whom little is gained by defining radiographic pathology, should be treated with palliative measures and not be subjected to painful, unnecessary testing. Before examination, pain should be treated so that patients are comfortable and able to complete their radiographic procedures. There are several ways of managing the more common dose-limiting symptoms (Table 4). The most feared side effect is respiratory depression, which fortunately is uncommon. Respiratory depression from opioids is nearly always associated with sedation and miosis. Naloxone is given only if sedation is accompanied by bradypnea and only in doses that reverse respiratory depression and not analgesia, if possible. Patients on sustainedrelease opioids or methadone might require a continuous infusion of naloxone at the dose that reversed respiratory depression, because the half-life of naloxone is 30 minutes. Some patients fail to achieve adequate analgesia despite dose escalation because of dose-limiting side effects. The term adjuvant analgesic describes a drug that has a primary indication other than pain but has analgesic properties with certain types of pain. Nonsteroidal anti-inflammatory drugs and acetaminophen are not adjuvants, whereas the antiseizure drug gabapentin is an adjuvant analgesic in the case of neuropathic pain. A dramatic reduction of pain can occur with adjuvant analgesics, precipitating opioid toxicity, and therefore close observation is necessary when adjuvants are initiated. Most adjuvants improve the therapeutic index of opioids but, unlike opioids, have a ceiling effect. Permanent end-organ damage can occur with certain adjuvant medications, unlike opioids. The serum level may be helpful in guiding titration, which is not the case with opioids. Acetaminophen is an alternative for those with a history of gastrointestinal bleeding or renal dysfunction, but it should be limited to 4 g daily because of the risk of liver toxicity.
Longer term therapy for hyperkalemia without conduction abnormalities should be directed toward minimizing intake and increasing excretion of potassium schedule 8 medications list cheap 500 mg panadol mastercard. Approximately 44% of new patients entering dialysis in the United States are diabetics. Early diagnosis of diabetes and early intervention are critical in preventing the normal progression to renal failure seen in many type 1 and a significant percentage of type 2 diabetics. The prevalence of diabetes is higher in certain racial and ethnic groups, affecting approximately 13% of African Americans, 9. Renal disease is suspected to be secondary to diabetes in the clinical setting of long-standing diabetes. This is supported by the history of diabetic retinopathy, particularly in type 1 diabetics, in whom there is a strong correlation. The natural history of diabetic nephropathy is a process that progresses gradually over years. This is believed to be related to increased cell growth and expansion in the kidneys, possibly mediated by hyperglycemia itself. Overt nephropathy, with urinary protein excretion higher than 300 mg/day, often develops after 10 to 15 years. Patients often present at diagnosis with microalbuminuria because of delays in diagnosis and other factors affecting protein excretion. Because of the high prevalence of type 2 compared with type 1 diabetes, however, most diabetics on dialysis are type 2 diabetics. Long-standing hyperglycemia is known to be a significant risk factor for the development of diabetic nephropathy. Hyperglycemia may directly result in mesangial expansion and injury by an increase in the mesangial cell glucose concentration. The glomerular mesan- gium expands initially by cell proliferation and then by cell hypertrophy. Increased mesangial stretch and pressure can stimulate this expansion, as can high glucose levels. Proteinuria, a marker and potential contributor to renal injury, accompanies diabetic nephropathy. Increased glomerular permeability will allow plasma proteins to escape into the urine. Some of these proteins will be taken up by the proximal tubular cells, which can initiate an inflammatory response that contributes to interstitial scarring eventually leading to fibrosis. Tubulointerstitial fibrosis is seen in advanced stages of diabetic nephropathy and is a better predictor of renal failure than glomerular sclerosis. There is an epithelial-mesenchymal transition that takes place in the tubules, with proximal tubular cell conversion to fibroblast-like cells. These cells can then migrate into the interstitium and produce collagen and fibronectin.
Kew (Kava). Panadol.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96842
It produces responses in approximately 50% of patients and a progression-free survival of approximately 15 months medicine daughter lyrics cheap panadol 500 mg on line. A meta-analysis comparing combination chemotherapy with melphalan and prednisone has shown no statistically significant difference in survival, despite a higher response rate with moreaggressive combination chemotherapy. Despite this finding, the combination of melphalan and prednisone was abandoned as induction therapy, because long-term therapy with alkylating agents compromises the ability to collect stem cells for high-dose therapy and stem This includes disappearance of all evidence of serum and urine Mcomponents on electrophoresis as well as by immunofixation studies for 6 weeks. Although the response rates are exciting, survival data for these new combinations remains immature. In summary, the optimal first-line therapy remains undefined but likely involves a combination of a novel agent (lenalidomide, thalidomide, or bortezomib) and corticosteroids. A more intensive approach is likely to result in a higher response rate, but this may be offset by a greater likelihood of significant toxicity, and treatment should be individualized. The patient is then given high-dose chemotherapy (usually melphalan, 200 mg/m2) as the high-dose preparative regimen of choice. Patients randomized to standard therapy in this study had similar response rates as patients who received highdose therapy, thus implying that a response achieved with either therapy has similar prognostic implications. The combinations of novel therapies in patients with newly diagnosed myeloma often result in high responses rates, similar to those achieved with highdose therapy. Accordingly, the precise role of high-dose therapy in the era of novel agents with high response rates remains to be determined. In vitro purging of peripheral stem cells has not been demonstrated to result in superior outcomes and is not routinely recommended. Alternatively, in vivo purging of stem cells by induction chemotherapy before stem cell collection is believed to be beneficial. Tandem Autologous Stem Cell Transplantation the success of high-dose therapy followed by peripheral blood stem cell transplantation has prompted French investigators to evaluate tandem autologous stem cell transplantation. Patients were subsequently randomized to receive a single autologous stem cell transplant with melphalan 140 mg/m2 and total body irradiation or a tandem autologous stem cell transplant; the first transplant consisted of melphalan 140 mg/m2 alone, and the second consisted of melphalan 140 mg/m2 with total body irradiation. Patients must also have a decrease by 50% in the size of soft tissue plasmacytoma. If serum and urine M protein are not measurable, a 50% or greater decreased in the difference of the involved and uninvolved free light chain. A 25% to 49% reduction in the size of soft tissue plasmacytoma must be demonstrated. Plateau Phase (P) A stable serum and urine paraprotein (within 25%) maintained for at least 3 months.
Stretching treatment 002 effective 500mg panadol, tearing, or contusion of these tissues can occur after sudden unexpected force applied to the spine from events such as heavy lifting, torsion of the spine, and whiplash injury. Routine spine radiographs are of limited value because they visualize only bony structures. First, it is necessary to determine whether the symptoms are caused by nerve root involvement. Second, it is necessary to determine whether the acute or chronic spine pain is related to a serious underlying medical illness that is manifesting itself as spine pain. After an initial assessment of the likely cause of the symptoms, the spine pain can then be treated. AcuteNonspecificBackPain There is general agreement that patients with acute nonspecific spine pain or nonlocalizable lumbosacral radiculopathy (without neurologic signs or significant neurologic symptoms) require only conservative medical management. Patients should abstain from heavy lifting or other activities that aggravate the pain. Recommended medications include nonsteroidal antiinflammatory drugs such as ibuprofen or aspirin. If there are complaints of muscle spasm, muscle relaxants such as cyclobenzaprine may be used in the acute phase of pain. Narcotic analgesia should be avoided, in general, but it can be prescribed in cases of severe acute pain. A study by Cherkin and coworkers compared standard physical therapy maneuvers and chiropractic spinal manipulation for the treatment of acute low back pain and found that both provide small short-term benefits and improve patient satisfaction, but they increase the cost of medical care and do not decrease the recurrence of back pain. Nerve conduction studies are indicated primarily to exclude other neuromuscular disorders that can mimic radiculopathy, such as peripheral polyneuropathy and mononeuropathies. The H-reflex can be a useful nerve conduction study when assessing for the presence of an S1 radiculopathy. The needle electrode examination is most likely to be useful in the presence of clinical weakness. This procedure will help distinguish weakness due to spinal nerve root damage from other causes of weakness identified on the physical examination, such as other neuromuscular disorders, central nervous system disorders, and non-neurologic causes of weakness (pain, malingering). The needle electrode examination should be performed only after at least 3 weeks have passed since the onset of weakness because fibrillation potentials (the major manifestation of acute denervation) do not reliably develop before that time. Electrodiagnostic testing may be of value in the assessment of patients with postsurgical deficits, multisegmental neurologic deficits, or multilevel intraspinal structural changes. Such patients present with complicated clinical and neuroimaging evidence, and electrodiagnostic testing might clarify issues of the location, activity, and severity of spinal nerve root disease.
Perinatal death is variable and can reach 37% when the syndrome occurs at an earlier stage of pregnancy medications similar to lyrica generic panadol 500mg with visa. It also improves biochemical markers without adversely affecting the mother or the baby. High levels of bile acids have been implicated in premature labor, meconium staining and sudden death. It is characterized by severe nausea and vomiting, with electrolyte disturbances that can require hospitalization. The outcome for the mother is benign except when severe vomiting causes esophageal rupture, vascular depletion, and renal damage. Adverse infant outcomes such as prematurity and low birth weight are rare and seem to occur because of poor maternal weight gain later in the pregnancy. Generalized pruritus is the main complaint, and jaundice occurs in up to 50% of cases. There are no clinical markers that predict the course of a pregnancy and the pathophysiologic mechanisms are not always understood, but knowledge and management of the preconception liver disease and efficacious pre-pregnancy and prenatal care are essential. A coordinated team approach that involves the primary care physician, obstetrician, hepatologist, and transplant surgeon is often required to promote good maternal and fetal outcomes. Zapata R, Sandoval L, Palma J, et al: Ursodeoxycholic acid in the treatment of intrahepatic cholestasis of pregnancy. Intervention might not be required except in cases of viral hepatitis E and herpes simplex hepatitis. Women with well-compensated cirrhosis and noncirrhotic portal hypertension may become pregnant. Preconception care and management of pregnant women with portal hypertension should be similar to that for nonpregnant women. Fertility may be restored after liver transplantation and pregnancy might have a good outcome. Vigilance in recognizing liver disorders in pregnancy and early coordinated management among the primary care physician, obstetrician, liver specialist, and transplant surgeon are essential for promoting good maternal and fetal outcomes. Preoperative recipient factors such as age older than 60 years, presence of comorbid conditions such as cardiac or pulmonary disease, renal failure, diabetes, and severe malnutrition, and the nature of the liver disease can affect survival. Perioperative factors such as the quality of the donor liver, difficulty of the liver transplantation procedure, development of postoperative infection, and side effects of immunosuppressive agents are important factors influencing outcome. Patients with end-stage liver disease undergo extensive workups before being listed for liver transplantation. The preoperative condition, nature and severity of the liver disease, and comorbid conditions are assessed during the evaluation process. Patients are presented and discussed in a multidisciplinary committee to be approved for final listing. Similarly, if the hepatic artery is unsuitable for revascularization of the transplanted liver, an arterial conduit from the aorta may be required.
National Guideline Clearinghouse: Diagnosis and treatment of diabetic foot infections treatment 1st degree av block panadol 500mg with amex, 2008. Suggested Readings American Diabetes Association: Consensus development conference on diabetic foot wound care. ArterialUlcers In regard to arterial ulcers, a vascular medicine or surgery specialist should be consulted. The prevalence of childhood and adolescent obesity has tripled since 1980 and, currently, 17% of U. Obesity and morbid obesity affect women and minorities (particularly middle-aged black and Hispanic women) more than white males. However, in almost every age and ethnic group, the prevalence of overweight or obesity exceeds 50%. Recent studies have also delineated the importance of childhood weight for influencing adulthood weight. Being overweight during older childhood is highly predictive of adult obesity, especially if a parent is also obese. Being overweight during the adolescent years is an even greater predictor of adult obesity. Obesity is now the second leading cause of preventable death after cigarette smoking, despite expenditures of over $45 billion annually on weight loss products. Increased abdominal fat raises the intra-abdominal pressure and contributes to gastroesophageal reflux, stress urinary incontinence, venous stasis disease, and abdominal hernia in obese patients. Excess weight causes joint and back stress that can lead to debilitating joint disease. The low-grade inflammatory state associated with morbid obesity has been implicated in the development of vascular and coronary artery disease and the hypercoagulable state seen in these patients. Obese patients have impaired pulmonary function, particularly decreased functional residual capacity, and frequently suffer from asthma, obstructive sleep apnea, and obesity hypoventilation syndrome (pickwickian syndrome). Other comorbidities include hypertension, dyslipidemia, asthma, and sex hormone dysfunction. Obesity is associated with an increased incidence of uterine, breast, ovarian, prostate, and colon cancer and of skin infections, urinary tract infections, migraine headaches, depression, and pseudotumor cerebri. A thorough history, physical examination, and focused testing will uncover previously undiagnosed comorbidities in up to two thirds of obese patients. The pretreatment evaluation performed at the Cleveland Clinic is consistent with published guidelines. Cardiology evaluation is carried out when there is evidence of cardiac disease based on clinical symptoms or electrocardiographic findings. Chest radiography and baseline laboratory testing, including a complete blood count, chemistry panel, liver function tests, thyroid function tests, and a lipid profile, should be performed as well.
Bozep, 29 years: Several studies have evaluated different agents thought to be capable of reducing the risk of prostate cancer. Etiology of cirrhosis in pregnancy is similar to that in the nonpregnant state and commonly includes alcohol and viral hepatitis C and B.
Finley, 33 years: Neurologic findings such as unexplained peripheral neuropathy or dementia are suggestive. Adjuvant radiation therapy decreases the rate of local recurrence, whereas the addition of systemic chemotherapy further enhances local control and improves survival.
Luca, 53 years: These disorders have been suggested to represent a spectrum of the same pathologic mechanisms, making the differentiation among them challenging. However, unvaccinated adults typically receive this vaccine only when they expect high-risk exposure to blood or body fluids.
Eusebio, 45 years: Pain usually courses in the distribution of the motor, sensory, or autonomic nerve, except when pain is funicular. Progressive disseminated histoplasmosis: this can be treated with liposomal amphotericin B (3-5 mg/kg/day), changing to intraconazole (200 mg three times daily � 3 days and then twice daily) if there is initial response.
Mortis, 46 years: Certain alleles, such as the S allele, either in the homozygous state or associated with the M allele, do not appear to be associated with the abnormally polymerized molecules within the endoplasmic reticulum and have not been incriminated in the development of liver or lung disease unless combined with the Z allele. Recent literature has supported an association of pityriasis rosea with human herpesvirus-6 and -7.
Kaffu, 63 years: Treatment includes shampoo for the scalp, such as those containing zinc pyrithione, selenium sulfide, or ketoconazole, and a mild topical corticosteroid. The amount8-10 and source10,11 of carbohydrates are important determinants of postprandial glucose.
Onatas, 51 years: When mucosal breaks are present, the patient is classified as having erosive esophagitis. Ecthyma can evolve from a primary pyoderma, in a pre-existing dermatosis, or at the site of trauma.
Musan, 24 years: In mild disease, an early cholecystectomy performed during the same hospitalization is favored. The polymerase chain reaction assay may be useful in the first week, and has a sensitivity rate of 67% to 87% and a specificity of approximately 100%.
References