




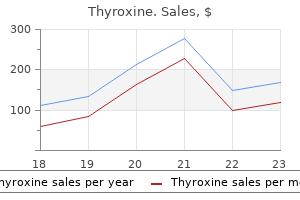
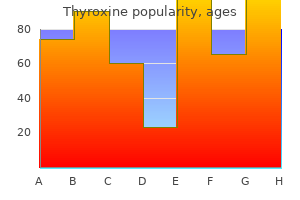
Stephen P. Glasser, MD
Thyroxine dosages: 200 mcg, 125 mcg, 100 mcg, 75 mcg, 50 mcg, 25 mcg
Thyroxine packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills, 100 pills, 200 pills, 300 pills

Quetiapine extended release symptoms 8 days past ovulation buy discount thyroxine 100mcg online, olanzapine, risperidone, and lamotrigine have been approved for maintenance treatment as sole agents, in combination with lithium and with aripiprazole and ziprasidone as adjunctive drugs. Lurasidone, olanzapine/fluoxetine, and quetiapine are also approved to treat acute depressive episodes in bipolar disorder. Compliance is frequently an issue and often requires enlistment and education of concerned family members. Efforts to identify and modify psychosocial factors that may trigger episodes are important, as is an emphasis on lifestyle regularity. Antidepressant medications are sometimes required for the treatment of severe breakthrough depressions, but their use should generally be avoided during maintenance treatment because of the risk of precipitating mania or accelerating the cycle frequency. Loss of efficacy over time may be observed with any of the mood-stabilizing agents. In such situations, an alternative agent or combination therapy is usually helpful. Personality factors may be a significant risk factor, as may a low level of educational or socioeconomic status or a history of recent stressful life events. Cultural factors are relevant as well and should be incorporated into the evaluation. Individuals who have persistent preoccupations about having or acquiring a serious illness, but who do not have a specific somatic complaint, may qualify for a related diagnosis-illness anxiety disorder. The diagnosis of conversion disorder (functional neurologic symptom disorder) is used to specifically identify those individuals whose somatic complaints involve one or more symptoms of altered voluntary motor or sensory function that cannot be medically explained and that causes significant distress or impairment or requires medical evaluation. In factitious illnesses, the patient consciously and voluntarily produces physical symptoms of illness. A variety of signs, symptoms, and diseases have been either simulated or caused by factitious behavior, the most common including chronic diarrhea, fever of unknown origin, intestinal bleeding or hematuria, seizures, and hypoglycemia. In malingering, the fabrication derives from a desire for some external reward such as a narcotic medication or disability reimbursement. There is usually no specific aversion to food in general but a preferential choice to ingest substances such as clay, starch, soap, paper, or ash. The diagnosis requires the exclusion of specific culturally approved practices and has not been commonly found to be caused by a specific nutritional deficiency. Onset is most common in childhood but the disorder can occur in association with other major psychiatric conditions in adults. An association with pregnancy has been observed, but the condition is only diagnosed when medical risks are increased by the behavior. The behavior typically occurs on a daily basis and must persist for at least 1 month.
Public House Plant (Asarabacca). Thyroxine.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96833
Moreover medicine man movie cheap thyroxine 150 mcg otc, it is well-tolerated, and the dosing schedule of monthly intravenous infusions makes it very convenient for patients. Conversely, in patients who have these antibodies (especially those who have them in high titer), the risk may be as high as 0. The risk is also high in patients who have previously received immunosuppressive therapy. A small percentage (<10%) of patients experience hypersensitivity reactions (including anaphylaxis), and 6% develop neutralizing antibodies to the molecule (only half of which persist). After this time, in antibody-positive patients, a change to another diseasemodifying therapy should be strongly considered. By contrast, persistently antibody-negative patients can be continued on treatment indefinitely. Fingolimod Fingolimod is a sphingosine-1-phosphate (S1P) inhibitor that prevents the egress of lymphocytes from the secondary lymphoid organs such as the lymph nodes and spleen. It is well tolerated, and the daily oral dosing schedule makes it very convenient for patients. However, its relative efficacy compared to other agents has not been established conclusively. First- and seconddegree heart block and bradycardia can also occur when fingolimod therapy is initiated. A 6-h period of observation (including electrocardiogram monitoring) is recommended for all patients receiving their first dose, and individuals with preexisting cardiac disease should probably not be treated with this agent. However, its twice-daily oral dosing schedule makes it somewhat less convenient for patients than daily oral therapies. Gastrointestinal side effects (abdominal discomfort, nausea, vomiting, flushing, and diarrhea) are common at the start of therapy but generally subside with continued administration. Other adverse events included mild decreases in neutrophil and lymphocyte counts and mild elevations in liver enzymes. Nevertheless, these reports underscore the fact, stated previously, that long-term safety can never be guaranteed by the results of short-term trials. Teriflunomide Teriflunomide inhibits the mitochondrial enzyme dihydro-orotate dehydrogenase, which is a key part of the pathway for de novo pyrimidine biosynthesis from carbamoyl phosphate and aspartate. It is well tolerated, and its daily oral dosing schedule makes it very convenient for patients. In the pivotal clinical trials, mild hair thinning and gastrointestinal symptoms (nausea and diarrhea) were more common than in controls, but in general, treatment with teriflunomide was well tolerated. As with any new agent, the long-term safety is not guaranteed by the results of short-term trials. A major limitation, especially in women of childbearing age, is its possible teratogenicity (pregnancy category X); teriflunomide can remain in the bloodstream for 2 years, and it is recommended that exposed men and women who wish to conceive receive cholestyramine or activated charcoal to eliminate residual drug.
Susceptibility-weighted imaging treatment 02 academy order 100 mcg thyroxine otc, such as gradient echo imaging, is very sensitive to magnetic susceptibility generated by blood, calcium, and air and routinely obtained in patients suspected of pathology that might result in microhemorrhages, such as amyloid, hemorrhagic metastases, and thrombotic states. Images are made by computerized processing of resonance information received from protons in the body. Coronal postcontrast T1-weighted image demonstrates a ring-enhancing mass in the left frontal lobe. Axial diffusion-weighted image demonstrates restricted diffusion (high signal intensity) within the lesion, which in this setting is highly suggestive of cerebral abscess. Gadolinium is a paramagnetic substance, which means that it reduces the T1 and T2 relaxation times of nearby water protons, resulting in a high signal on T1W images and a low signal on T2W images (the latter requires a sufficient local concentration, usually in the form of an intravenous bolus). These differ according the attached chelated moiety, which also affects the strength of chelation of the otherwise toxic gadolinium element. The chelating carrier molecule for gadolinium can be classified by whether it is macrocyclic or has linear geometry and whether it is ionic or nonionic. Cyclical agents are less likely to release the gadolinium element, and thus are considered the safest category. The agents are generally well tolerated; overall adverse events after injection range from 0. Severe life-threatening reactions are exceedingly rare; in one report, only 55 reactions out of 20 million doses occurred. However, the adverse reaction rate in patients with a prior history of reaction to gadolinium is eight times higher than normal. Gadolinium contrast material can be administered safely to children as well as adults, although these agents are generally avoided in those under 6 months of age. In addition to dermatologic symptoms, other manifestations include widespread fibrosis of the skeletal muscle, bone, lungs, pleura, pericardium, myocardium, kidney, muscle, bone, testes, and dura. A history of renal disease (including solitary kidney, renal transplant, renal tumor) 2. The patient lies on a table that is moved into a long, narrow gap within the magnet. Coronal (A) and axial (B) T2-weighted fluid-attenuated inversion recovery images demonstrate expansion and high signal intensity involving the right medial temporal lobe and insular cortex (arrows). Coronal diffusion-weighted image demonstrates high signal intensity indicating restricted diffusion involving the right medial temporal lobe and hippocampus (arrows) as well as subtle involvement of the left inferior temporal lobe (arrowhead). This is most consistent with neuronal death and can be seen in acute infarction as well as encephalitis and other inflammatory conditions. The suspected diagnosis of herpes simplex encephalitis was confirmed by cerebrospinal fluid polymerase chain reaction analysis.

Thus medications knee cheap thyroxine 200 mcg overnight delivery, the first step is a thorough physical examination in all alcoholics considering abstinence, including a search for evidence of liver failure, gastrointestinal bleeding, cardiac arrhythmia, infection, and glucose or electrolyte imbalances. Short-half-life benzodiazepines can be considered for patients with serious liver impairment or evidence of significant brain damage, but they must be given every 4 h to avoid abrupt blood-level fluctuations that may increase the risk for seizures. Aggressive behavior should be handled by offering reassurance but also by considering a possible show of force with an intervention team. If the aggressive behavior continues, relatively low doses of a short-acting benzodiazepine such as lorazepam. During motivational interviewing, the clinician helps the patient to think through the assets. Patients should be reminded that only they can decide to avoid 2728 4 or 5 days, these patients should return daily for evaluation of vital signs and can be hospitalized if signs and symptoms of withdrawal escalate. The focus of care is to identify and correct medical problems and to control behavior and prevent injuries. Many clinicians recommend the use of high doses of a benzodiazepine (as much as 800 mg/d of chlordiazepoxide has been reported), a treatment that will decrease agitation and raise the seizure threshold but probably does little to improve the confusion. Antipsychotics are less likely to exacerbate confusion but may increase the risk of seizures; they have no place in the treatment of mild withdrawal symptoms. Generalized withdrawal seizures rarely require more than giving an adequate dose of benzodiazepines. There is little evidence that anticonvulsants such as phenytoin or gabapentin are more effective in drug-withdrawal seizures, and the risk of seizures has usually passed by the time effective drug levels are reached. The core of treatment uses cognitive-behavioral approaches to help patients recognize the need to change, while working with them to alter their behaviors to enhance compliance. A key step is to optimize motivation toward abstinence through education about alcoholism and instructions to family members to stop protecting the patient from problems caused by alcohol. A third component, relapse prevention, helps the patient identify situations in which a return to drinking is likely, formulate ways of managing these risks, and develop coping strategies that increase the chances of a return to abstinence if a slip occurs. Whatever the setting, subsequent contact with outpatient treatment staff should be maintained for at least 6 months and preferably a year after abstinence. The physician serves an important role in identifying the alcoholic, diagnosing and treating associated medical and psychiatric syndromes, overseeing detoxification, referring the patient to rehabilitation programs, providing counseling, and, if appropriate, selecting which (if any) medication might be needed. For insomnia, patients should be reassured that troubled sleep is normal after alcohol withdrawal and will improve over subsequent weeks.
Although as many as one-half of patients in an intensive care setting are reported to have calcium concentrations of <2 symptoms youre pregnant cheap 25 mcg thyroxine with visa. Alkalosis increases calcium binding to proteins, and in this setting, direct measurements of ionized calcium should be made. Medications such as protamine, heparin, and glucagon may cause transient hypocalcemia. These forms of hypocalcemia are usually not associated with tetany and resolve with improvement in the overall medical condition. The hypocalcemia after repeated transfusions of citrated blood usually resolves quickly. Patients with acute pancreatitis have hypocalcemia that persists during the acute inflammation and varies in degree with disease severity. Occasionally, a chronic low total calcium and low ionized calcium concentration are detected in an elderly patient without obvious cause and with a paucity of symptoms; the pathogenesis is unclear. Neuromuscular and neurologic manifestations of chronic hypocalcemia include muscle spasms, carpopedal spasm, facial grimacing, and, in extreme cases, laryngeal spasm and convulsions. Increased intracranial pressure occurs in some patients with long-standing hypocalcemia, often in association with papilledema. Symptoms of untreated hypocalcemia are shared by both types of hypoparathyroidism, although the onset of hereditary hypoparathyroidism can be more gradual and associated with other developmental defects. Basal ganglia calcification and extrapyramidal syndromes are more common and earlier in onset in hereditary hypoparathyroidism. In previous decades, acquired hypoparathyroidism secondary to surgery in the neck was more common than hereditary hypoparathyroidism, but the frequency of surgically induced parathyroid failure has diminished as a result of improved surgical techniques that spare the parathyroid glands and increased use of nonsurgical therapy for hyperthyroidism. Genetic Abnormalities and Hereditary Hypoparathyroidism Hereditary hypoparathyroidism can occur as an isolated entity without other endocrine or dermatologic manifestations. Hereditary hypoparathyroidism is often manifest within the first decade but may appear later. Genetic defects associated with hypoparathyroidism serve to illuminate the complexity of organ development, hormonal biosynthesis and secretion, and tissue-specific patterns of endocrine effector function. Often, hypoparathyroidism is isolated, signifying a highly specific functional disturbance. When hypoparathyroidism is associated with other developmental or organ defects, treatment of the hypocalcemia can still be effective. A form of hypoparathyroidism associated with defective development of both the thymus and the parathyroid glands is termed the DiGeorge syndrome, or the velocardiofacial syndrome. Congenital cardiovascular, facial, and other developmental defects are present, and patients may die in early childhood with severe infections, hypocalcemia and seizures, or cardiovascular complications. Most cases are sporadic, but an autosomal dominant form involving microdeletions of chromosome 22q11. Smaller deletions in chromosome 22 are seen in incomplete forms of the DiGeorge syndrome, appearing in childhood or adolescence, that are manifest primarily by parathyroid gland failure. Deletions of the orthologous mouse gene show a phenotype similar to the human syndrome.

Among these symptoms of anemia purchase thyroxine 25mcg overnight delivery, pancreatic -cell glucagon, which stimulates hepatic glycogenolysis, plays a primary role. Adrenomedullary epinephrine, which stimulates hepatic glycogenolysis and gluconeogenesis (and renal gluconeogenesis), is not normally critical. When hypoglycemia is prolonged beyond 4 h, cortisol and growth hormone also support glucose production and restrict glucose utilization to a limited amount (20% compared to epinephrine). Thus cortisol and growth hormone play no role in defense against acute hypoglycemia. As plasma glucose levels fall further, symptoms prompt behavioral defense against hypoglycemia, including the ingestion of food (Table 420-2;. The normal glycemic thresholds for these responses to decreasing plasma glucose concentrations are shown in Table 420-2. They shift to higher-thannormal glucose levels in people with poorly controlled diabetes, who can experience symptoms of hypoglycemia when their glucose levels decline toward the normal range (pseudohypoglycemia). On the other hand, thresholds shift to lower-than-normal glucose levels in people with recurrent hypoglycemia;. Clinical Manifestations Neuroglycopenic manifestations of hypoglycemia are the direct result of central nervous system glucose deprivation. In insulindeficient diabetes, the key counterregulatory responses-suppression of insulin and increases in glucagon-are lost, and stimulation of sympathoadrenal outflow is attenuated. They include adrenergic symptoms (mediated largely by norepinephrine released from sympathetic postganglionic neurons but perhaps also by epinephrine released from the adrenal medullae), such as palpitations, tremor, and anxiety, as well as cholinergic symptoms (mediated by acetylcholine released from sympathetic postganglionic neurons), such as sweating, hunger, and paresthesias. Heart rate and systolic blood pressure are typically increased but may not be raised in an individual who has experienced repeated, recent episodes of hypoglycemia. Etiology and Pathophysiology Hypoglycemia is most commonly a result of the treatment of diabetes. This topic is therefore addressed before other causes of hypoglycemia are considered. Second, it precludes maintenance of euglycemia over a lifetime of diabetes and thus full realization of the well-established microvascular benefits of glycemic control. Third, it causes a vicious cycle of recurrent hypoglycemia by producing hypoglycemia-associated autonomic failure-i. They suffer an average of two episodes of symptomatic hypoglycemia per week and at least one episode of severe, at least temporarily disabling hypoglycemia each year.
Syndromes
Infectious diseases that can present with ataxia are meningovascular syphilis and tabes dorsalis due to degeneration of the posterior columns and spinocerebellar pathways in the spinal cord atlas genius - symptoms cheap thyroxine 200mcg without prescription. These lesions typically produce cerebellar symptoms ipsilateral to the injured cerebellum and may be associated with an impaired level of consciousness due to brainstem compression and increased intracranial pressure; ipsilateral pontine signs, including sixth and seventh nerve palsies, may be present. Focal and worsening signs of acute ataxia should also prompt consideration of a posterior fossa subdural hematoma, bacterial abscess, or primary or metastatic cerebellar tumor. Many of these lesions represent true neurologic emergencies, as sudden herniation, either rostrally through the tentorium or caudal herniation of cerebellar tonsils through the foramen magnum, can occur and is usually devastating. The clinical picture may be homogeneous within a family with dominantly inherited ataxia, but sometimes most affected family members show one characteristic syndrome, while one or several members have an entirely different phenotype. Although the phenotype is variable for any given disease gene, a pattern of neuronal loss with gliosis is produced that is relatively unique for each ataxia. Although the clinical manifestations and neuropathologic findings of cerebellar disease dominate the clinical picture, there may also be characteristic changes in the basal ganglia, brainstem, spinal cord, optic nerves, retina, and peripheral nerves. In large families with dominantly inherited ataxias, many gradations are observed from purely cerebellar manifestations to mixed cerebellar and brainstem disorders, cerebellar and basal ganglia syndromes, and spinal cord 2628 are descendants of a common ancestor, and the population may be the largest homogeneous group of patients with ataxia yet described. The gait is slow and stiff, with a slightly broadened base and lurching from side to side; this gait results from spasticity, not true ataxia. Of note is the prominence of horizontal and vertical nystagmus, loss of fast saccadic eye movements, hypermetric and hypometric saccades, and impairment of upward vertical gaze. Facial fasciculations, facial myokymia, lingual fasciculations without atrophy, ophthalmoparesis, and ocular prominence are common early manifestations. Ophthalmoparesis, upward vertical gaze deficits, and facial and lingual fasciculations are also present. Distal sensory loss involving pain, touch, vibration, and position senses and distal atrophy are prominent, indicating the presence of peripheral neuropathy. The deep tendon reflexes are depressed to absent, and there are no corticospinal or extrapyramidal findings. The major pathologic findings are variable loss of neurons and glial replacement in the corpus striatum and severe loss of neurons in the pars compacta of the substantia nigra. A moderate loss of neurons occurs in the dentate nucleus of the cerebellum and in the red nucleus. Cell loss also occurs in the dentate nucleus and in the cranial nerve motor nuclei.

Secondary iron overload occurs as a result of an iron-loading anemia medicine mound texas order thyroxine 50 mcg otc, such as thalassemia or sideroblastic anemia, in which erythropoiesis is increased but ineffective. In the acquired iron-loading disorders, massive iron deposits in parenchymal tissues can lead to the same clinical and pathologic features as in hemochromatosis. It is most common in populations of northern European extraction in whom approximately 1 in 10 persons are heterozygous carriers and 0. However, expression of the disease is variable and modified by several factors, especially alcohol consumption and dietary iron intake, blood loss associated with menstruation and pregnancy, and blood donation. Presumably there are as yet unidentified modifying genes responsible for expression and there is some early evidence to support this. Nearly 70% of untreated patients develop the first symptoms between ages 40 and 60. The disease is rarely evident before age 20, although with family screening (see "Screening for Hemochromatosis," below) and periodic health examinations, asymptomatic subjects with iron overload can be identified, including young menstruating women. The iron-storage pigment in tissues is called hemosiderin because it was believed to be derived from the blood. The term hemosiderosis is used to describe the presence of stainable iron in tissues, but tissue iron must be quantified to assess body-iron status accurately (see below and Chap. Hemochromatosis refers to a group of genetic diseases that predispose to iron overload, potentially leading to fibrosis and organ failure. Cirrhosis of the liver, diabetes mellitus, arthritis, cardiomyopathy, and hypogonadotropic hypogonadism are the major clinical manifestations. Although there is debate about definitions, the following terminology is widely accepted. Homozygosity for H63D is not associated with clinically significant iron overload. Mutations in the genes encoding hepcidin, transferrin receptor 2 (TfR2), and hemojuvelin. However, mutations in ferroportin, responsible for the efflux of iron from enterocytes and most other cell types, result in iron loading of reticuloendothelial cells and macrophages as well as parenchymal cells. In hemochromatosis, mucosal absorption is greater than body requirements and amounts to 4 mg/d or more. The progressive accumulation of iron increases plasma iron and saturation of transferrin and results in a progressive increase of plasma ferritin. A liver-derived peptide, hepcidin, represses basolateral iron transport in the intestine and iron release from macrophages and other cells by binding to ferroportin. Thus, hepcidin is a crucial molecule in iron metabolism, linking body stores with intestinal iron absorption. In advanced disease, the body may contain 20 g or more of iron that is deposited mainly in parenchymal cells of the liver, pancreas, and heart.
Indeed symptoms anemia discount thyroxine 25mcg on line, hypercalcemia may be noted incidentally during the workup of a patient with known or suspected malignancy. Clinical suspicion that malignancy is the cause of the hypercalcemia is heightened when there are other signs or symptoms of a paraneoplastic process such as weight loss, fatigue, muscle weakness, or unexplained skin rash, or when symptoms specific for a particular tumor are present. Bone scans with technetium-labeled bisphosphonate are useful for detection of osteolytic metastases; the sensitivity is high, but specificity is low; results must be confirmed by conventional x-rays to be certain that areas of increased uptake are due to osteolytic metastases per se. The stated upper limit of safe dietary intake is 2000 U/d (50 g/d) in adults because of concerns about potential toxic effects of cumulative supraphysiologic doses. These recommendations are now regarded as too restrictive, because some estimates are that in elderly individuals in northern latitudes, 2000 U/d or more may be necessary to avoid vitamin D insufficiency. Hypercalcemia is usually controlled by restriction of dietary calcium intake and appropriate attention to hydration. These measures, plus discontinuation of vitamin D, usually lead to resolution of hypercalcemia. However, vitamin D stores in fat may be substantial, and vitamin D intoxication may persist for weeks after vitamin D ingestion is terminated. Such patients are responsive to glucocorticoids, which in doses of 100 mg/d of hydrocortisone or its equivalent usually return serum calcium levels to normal over several days; severe intoxication may require intensive therapy. Management of the hypercalcemia can often be accomplished by avoiding excessive sunlight exposure and limiting vitamin D and calcium intake. Alternatively, glucocorticoids in the equivalent of 100 mg/d of hydrocortisone or equivalent doses of glucocorticoids may help control hypercalcemia. The hypercalcemia associated with the syndrome was first recognized in England after fortification of milk with vitamin D. Standard therapies for hypercalcemia (discussed below) are applicable to patients with malignancy. Abnormal metabolism of the vitamin is usually acquired in association with a widespread granulomatous disorder. The regulation of 2478 but the connection between these defects and hypercalcemia were not described until later. Studies suggest that genetic mutations involving microdeletions at the elastin locus and perhaps other genes on chromosome 7 may play a role in the pathogenesis. Withdrawal of the vitamin is usually associated with prompt disappearance of the hypercalcemia and reversal of the skeletal changes. As in vitamin D intoxication, administration of 100 mg/d of hydrocortisone or its equivalent leads to a rapid return of the serum calcium to normal. Secondary hyperparathyroidism occurs not only in patients with renal failure but also in those with osteomalacia due to multiple causes (Chap. For both disorders, hypocalcemia seems to be the common denominator in initiating the development of secondary hyperparathyroidism.
The most commonly used opiates are diverted prescriptions for oxycodone and hydrocodone treatment effect buy thyroxine 100 mcg free shipping, followed by heroin and morphine, and-among health professionals-meperidine and fentanyl. Heroin is derived from morphine and acts as a prodrug that more readily penetrates the brain and is converted rapidly to morphine in the body. Two opiate maintenance treatment agents-methadone and buprenorphine-are also misused, but at substantially lower rates, and the partial opiate agonists such as butorphanol, tramadol, and pentazocine are misused even less frequently. Because the chemistry and general pharmacology of these agents are covered in major pharmacology texts, this chapter focuses on the neurobiology and pharmacology relevant to dependence and its treatments. Although the neurobiology of abuse involves all four of the known opiate receptors-mu, kappa, delta, and nociceptin/orphanin-this discussion focuses on the mu receptor, at which most of the clinically used opiates are active. The different functional activities of opiate receptors are summarized in Table 468e-1. Thus, opiates inhibit the activity of diverse and widely distributed neuronal types. The major effects of opiates, such as analgesia, sedation, and drug reinforcement are produced through this inhibition of neurons that belong to specific brain pathways. Many opiate actions are related to the specific neuroanatomic locations of mu receptors. The positive subjective effects of opioid drugs also include mu receptor desensitization and internalization, potentially related to stimulation of beta-arrestin signalizing pathways. Therefore, routes of administration that slowly increase opiate blood and brain levels, such as oral and transdermal routes, are effective for analgesia and sedation but do not produce an opiate "high" that follows smoking and intravenous routes. These effects are also reflective of genetic risk factors for developing opiate use disorder, with estimates of up to 50% of the risk for dependence due to polygenic inheritance. When large opiate doses saturate and activate all of its mu receptors, action potentials cease. When this direct inhibitory effect is sustained over weeks and months of opiate use, a secondary set of adaptive changes occur that lead to tolerance and withdrawal symptoms. Other contributors to withdrawal include deficits within the dopamine reward system. Upregulation of this system is involved in opiate tolerance, and when the opiate is removed, unopposed noradrenergic neurotransmission is involved in opiate withdrawal. Tolerance appears to be primarily a pharmacodynamic rather than pharmacokinetic effect, with relatively limited induction of cytochrome P450 or other liver enzymes. The metabolism of opiates occurs in the liver primarily through the cytochrome P450 systems of 2D6 and 3A4.
Bandaro, 31 years: Some of the released free fatty acids bind albumin before entering cells and are transported to other tissues, especially the liver. Ochronotic arthritis is heralded by pain, stiffness, and some limitation of motion of the hips, knees, and shoulders. The current consensus is that medical monitoring rather than surgical correction of hyperparathyroidism may be justified in certain patients. Due to their mechanism of action, each drug causes an increase in hepatic fat, the long-term consequences of which are unknown.
Ugo, 54 years: Mutation markers are now commercially available to identify carriers at risk in their families, which allows for precise identification of the genetic mutation for correct diagnosis and also for family planning. The somatostatin analogue octreotide can be used to suppress insulin secretion in sulfonylurea-induced hypoglycemia. A complete neurologic examination is performed to localize the anatomic site of stroke. X-linked adrenoleukodystrophy/ adrenomyeloneuropathy Other disorders of macromolecule catabolism and autophagy Representing a significant proportion of the inborn metabolic dementia spectrum, disorders of lysosomal function reflect anomalous macromolecule catabolism.
Dawson, 62 years: The diagnosis of conversion disorder (functional neurologic symptom disorder) is used to specifically identify those individuals whose somatic complaints involve one or more symptoms of altered voluntary motor or sensory function that cannot be medically explained and that causes significant distress or impairment or requires medical evaluation. Once a diagnosis of hyperplasia is established, all the glands must be identified. In advanced disease, the body may contain 20 g or more of iron that is deposited mainly in parenchymal cells of the liver, pancreas, and heart. The patient may have loss of sensation (numbness), altered sensation to touch (hyperpathia or allodynia), or uncomfortable spontaneous sensations (tingling, burning, or aching) (Chap.
Kalesch, 49 years: Almost 10 million head injuries occur annually in the United States, about 20% of which are serious enough to cause brain damage. Although most poisons have predictable doserelated effects, individual responses to a given dose may vary because of genetic polymorphism, enzymatic induction or inhibition in the presence of other xenobiotics, or acquired tolerance. Blurred vision results from changes in the water content of the lens and resolves as the hyperglycemia is controlled. Especially for the recessive and X-linked forms, a family history of myelopathy may be lacking.
Kadok, 46 years: Glucocorticoids are used widely in the treatment of a variety of disorders, including chronic lung disorders, rheumatoid arthritis and other connective tissue diseases, inflammatory bowel disease, and after transplantation. Hexacarbon exposure leads to covalent cross-linking between axonal neurofilaments that result in their aggregation, impaired axonal transport, swelling of the axons, and eventual axonal degeneration. Deep-brain stimulation of the region of the posterior hypothalamic gray matter has proven successful in a substantial proportion of patients, although its risk-benefit ratio makes it inappropriate with so many other options now available. The past decade has also witnessed the development of revolutionary new techniques-optogenetics and designer receptors and ligands-that provide unprecedented temporal and spatial control of neural circuits and permit detection of neural activity in real time in awake, behaving animals.
Gembak, 47 years: The serotonin precursor 5-hydroxitriptophan (plus carbidopa) may be useful in some cases of postanoxic myoclonus. Shellfish acquire these toxins by feeding on dinoflagellates, particularly of the genera Dinophysis and Prorocentrum. A definitive diagnosis of glycolytic disease is made by muscle biopsy and subsequent enzyme analysis or by genetic testing. When osteitis fibrosa cystica is severe, however, bone mineral deficits can be large.
Abe, 32 years: There is no motor component to the nerve, and therefore weakness is not a part of this syndrome. Hypertension is the most significant of the risk factors; in general, all hypertension should be treated to a target of less than 140� 150/90 mmHg. Agitation is an inappropriate and disruptive increase in activity, and may manifest as motoric (pacing, fidgeting, picking), verbal/vocal (shouting, cursing, grunting), or affective (anger, laughing, crying) symptoms. With these associations, it is not surprising that individuals with obstructive sleep apnea frequently have the metabolic syndrome.
References