




Catherine Cordonnier, M.D.
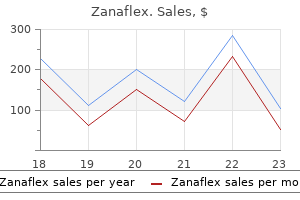
Zanaflex dosages: 4 mg, 2 mg
Zanaflex packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Phrynoderma has now been described in patients with normal vitamin A levels and has been associated with other nutritional deficiencies including including B complex muscle relaxant 25mg order 2 mg zanaflex fast delivery, ribofla vin, vitamin C, vitamin E, essential fatty acids and malnutrition [1]. History Phrynoderma starts gradually with mostly nonpruritic lesions on the elbows. The elbows and knees are the most commonly affected areas but the buttocks and extensor surfaces of the limbs may be affected. The con dition is usually associated with ocular signs, such as night blind ness, conjunctival xerosis and ulcerations [12]. Introduction and general description this is a rare condition first described in 1999 in immunocompro mised patients [1]. It is due to a novel polyoma virus that appears to infect keratinocytes of the inner root sheath of the hair follicle. Incidence and prevalence Trichodysplasia spinulosa is rare with only a small number of reported cases in the world literature. Age Trichodysplasia spinulosa has been reported in immunosup pressed patients of all age groups [2]. Complications and comorbidities Ocular involvement including the development of Bitot spots, conjunctival xerosis and blindness may be associated with phrynoderma. Associated diseases Most patients with trichodysplasia spinulosa are immunosup pressed following organ transplantation [3]. There have been rare reports of trichodysplasia spinulosa associated with sys temic lupus erythematosus [5]. Investigations All patients with phrynoderma should have their vitamin A levels measured. In some patients with nutritional deficiency, there will be con comitant hypoproteinaemia. In this circumstance, values of vita min A can appear reduced despite adequate vitamin A stores. Pathophysiology Management Treatment involves the correction of poor diet and administration of a multivitamin preparation containing vitamin A, since poor diet often results in other concurrent deficiencies. The dosage, in children aged 8 years or above and adults is 100 000 units daily for 3 days, followed by 50 000 units daily for 2 weeks, and then 10 000 units daily for 2 months, until liver storage is adequate [13].
These cases are usually without central nervous system abnormalities and are naevoid muscle relaxant and nsaid 2 mg zanaflex with mastercard. A case of unilateral lentiginosis with contralateral naevus depigmentosus has been reported [9]. Distribution of the lentigines included the face, lips, extremities, buttocks, palms and soles, but not mucosal surfaces. The condition is extremely common in lightskinned black people, especially in combination with reddishbrown hair [2]. Lentiginosis the histological and clinical features of lentigo, together with other lesions in which the number of melanocytes is increased, are fully described in Chapter 132. A lentigo is a benign pigmented macule in which there is an increased number of melanocytes. Genetic syndromes of which lentiginosis is a component are described in Chapter 70. It is well recognized in adolescents and young adults who show no evidence of systemic abnormalities but has also been linked to treatment with cancer chemotherapeutic agents and to immunosuppression, particularly in transplant recipients. In 1956, Degos and Carteaud described telangiectatic papules that darkened and evolved into depressed Generalized lentiginosis Lentigines are commonly multiple but appear singly or in small crops at irregular intervals from infancy onwards. A less common clinical pattern is localization of lentigines to sites previously affected by psoriasis, creating an appearance not unlike a naevus spilus [2]. Melanomas however tend to have more variation in colour density within the lesion than in lentigo. Note lentigines in different stages of evolution, particularly on the right wrist and the forearm. There is a dose effect with a tendency to a greater number of lentigines in those who have Addison disease Hyperpigmentation may be a cutaneous manifestation of Addison disease. Topical therapy including tretinoin and adapalene creams can be used to ameliorate the cutaneous manifestations. Pathology the hypermelanosis is the result of increased secretion of melanotrophic hormones by the pituitary. Absence of hypermelanosis in Addison disease was explained in a single case by a high degree of melanosome degradation in secondary lysosomes [1]. Cushing syndrome Definition Cushing syndrome is caused by excessive amounts of cortisol leading to obesity, a moonshaped face and increased fat deposition in the neck area. Presentation Increased pigmentation is such a wellknown feature of Addison disease that its absence may significantly delay diagnosis and endanger life [1,2]. When present, the hyperpigmentation of Addison disease is typically diffuse and is most intense on areas exposed to light [3].
Syndromes
Capillaritis (pigmented purpura) (see Chapter 101) Haemosiderosis without clinically evident hypermelanosis is seen in Schamberg capillaritis [4] muscle relaxant whole foods zanaflex 4 mg order without a prescription. Congenital haemolytic anaemia Conspicuous pigmentation of the lower leg in the third decade or earlier may develop in patients with sickle cell anaemia. Haemochromatosis the presence of haemosiderin stimulates melanogenesis, and hypermelanosis may dominate the clinical and histological picture, as in haemochromatosis (see earlier). Dermatitis Haemosiderosis of the trunk is a feature of some reactions to textiles. Small patches of haemosiderosis, most numerous on the lower legs but progressively involving the thighs and buttocks, are characteristic of drug reactions to anticonvulsants with a ureide structure, a property common to the majority of them. Jaundice and bronze baby syndrome Definition and nomenclature Jaundice: yellowish discoloration of the skin, eyes and mucous membranes due to deposition of bile pigments [1]. Unsurprisingly, all samples from pigmented skin showed a higher melanin content than those from unpigmented skin. This suggests that hypermelanosis may be provoked by chronic venous insufficiency itself without the requirement for extravascular erythrocyte destruction and haemosiderin [3]. Interestingly, in a study of 46 patients with various types of leg ulcer it was shown that haemosiderin could be detected in skin biopsies from all patients but that urinary haemosiderin, which was absent from all patients with ischaemic ulcers, could be detected 22 of 24 patients with venous ulcers [4]. There was, however, no correlation between the amounts deposited in the skin and the amount detected in urine. Disease course and prognosis Hypostatic haemosiderosis the pigmentation usually persists even if the venous insufficiency is relieved. Clinically, it is often first noticed in the sclerae, because bilirubin has affinity for elastic tissue. The range of yellow shades produced by bilirubin may be modified by the presence of biliverdin, which adds a greenish hue. Bronzing is the effect of added melanin pigmentation and is often seen in jaundice of long duration. However, it is now more commonly seen in young women drastically reducing their weight and eating foodstuffs with high carotene content [2,3]. Iatrogenic hypercarotenaemia occurs in patients on oral supplements of carotene as a photoprotective agent in erythropoietic protoporphyria [4,5] with or without canthaxanthine.
Age Onset is most commonly in adult life muscle relaxant methocarbamol zanaflex 2 mg buy on-line, typically in the fourth decade, though cases have been reported from childhood to old age [10]. Sex Several studies have suggested that dermatitis herpetiformis is commoner in men than women, with a male to female ratio of 1. Ethnicity It is largely a condition of people of northern European descent and is most uncommon in Asian and African populations, though occasional cases have been reported [12]. Interestingly, the incidence and prevalence of the disease is similar in North American populations of European descent to those seen in northern Europe, suggesting that genetic factors are important in disease susceptibility [11]. Dermatitis herpetiformis Definition and nomenclature Dermatitis herpetiformis is a chronic, intensely pruritic, skin condition associated with glutensensitive enteropathy. It results in deposition of IgA antitransglutaminase autoantibodies in the dermal papillae which lead to neutrophil infiltration and blister formation. Consequently, all patients with dermatitis herpetiformis should be reviewed by a gastroenterologist and investigated Dermatitis herpetiformis 50. An important consequence of a diagnosis of dermatitis herpetiformis is an increased risk of small bowel lymphoma [17]. Autoimmune diseases tend to associate with one another, presumably because of genetic susceptibility factors, and dermatitis herpetiformis is no different. The commonest association is with autoimmune thyroid disease [18,19], and all patients with dermatitis herpetiformis should be screened for this. Additionally, patients with dermatitis herpetiformis have increased risk of type 1 diabetes [20], Addison disease [21] and vitiligo [18]. The series of events that results in inflammation and itch in dermatitis herpetiformis remains to be fully elucidated [25,26]. Subsequently neutrophilic infiltration occurs, leading to inflammation and clefting within the lamina lucida. Patients report a rash, most typically over the extensor surfaces of the elbows, knees, buttocks and scalp. Because the condition is so pruritic, intact vesicles are rarely seen and the patient may simply present with excoriations [38]. Mucosal change may occur [41], and dental abnormalities have been reported, particularly enamel pits [42,43]. Other environmental factors relevant to dermatitis herpetiformis include iodine exposure (which can precipitate flares of the disease [35]) and tobacco smoking, which may ameliorate it [36,37]. Differential diagnosis the differential diagnosis of dermatitis herpetiformis includes many pruritic and vesiculobullous disorders including linear IgA disease, pemphigoid, eczema and scabies. Management There are no randomized clinical trials in the management of dermatitis herpetiformis.
The high prevalence of balding in the male population spasms rectum zanaflex 4 mg purchase amex, racial variation in the agerelated prevalence of balding, the finding that baldness androgenetic alopecia and pattern hair loss 89. Pre viously reported or hypothesized associations with smoking and benign prostatic hypertrophy were not confirmed [21]. Thus, those who do seek help are likely to be in greater emotional distress and to have been dissatisfied with any treatment they have received. The most distressed bald ing men are those with more extensive hair loss, those who have very early onset, and those who regard their balding as progres sive (often arising from observation of their father) and socially noticeable [63]. Female features the clinical presentation of pattern hair loss in women differs from men. Women may present with either an episodic or continuous increase in hair shedding without any noticeable reduction in hair volume, increased hair shedding with loss of hair volume over the crown, or diffuse thinning over the crown with no history of hair shedding [67]. The most informative question to ask balding women is about the change in the thickness of their ponytail. Loss of volume or thinning over the crown is best detected when the hair is parted centrally. Widening of the central parting may follow a Christmastree pat tern and is used to score the hair loss [68]. Stage 1 is normal hair density; stage 2 shows widening of the central part; stage 3 demonstrates additional thinning of the hair at the sides of the partline; stage 4 reflects the development of a bald patch distal to the anterior hairline; and stage 5 represents advanced hair loss. Bitemporal recession occurs in 13% of premenopausal women and 37% of postmenopausal women [70]. In many women the hair loss is confined to the scalp vertex, but in a significant proportion hair loss also occurs diffusely over the parietal scalp. Generalized hair loss often precludes women from hair transplantation proce dures because of a diminished donor population in the occipital region. However, if the hair loss is of sudden onset, rapidly progressive and advanced, a full medical history and examination, and endocrinological investigation, are desirable to exclude virili zation, which can rarely be caused by a virilizing tumour. In contrast to the prevailing attitude to male balding, society generally regards it as abnormal for women to lose their hair and the adverse effect of hair loss on quality of life tends be more severe in women than in men. As a group, women seek ing medical advice for their hair loss experience more negative body image feelings, more social anxiety and poorer selfesteem and psychosocial wellbeing than control subjects with non visible skin disease, as well as dissatisfaction with their hair. In Clinical features the essential clinical feature of balding in both sexes is patterned hair loss over the crown. Terminal hairs are progressively replaced by shorter, finer hairs which may also appear less pigmented. This process may begin at any age after the onset of adrenarche and may precede pubarche. Male features the clinical appearance of male balding is instantly recognizable in most cases.
Alcohol abstinence helped to induce remission and relapse was induced by re consumption spasms headache buy 2 mg zanaflex with visa. The effects of alcohol on immune function and skin vasculature are thought to precipitate exacerbations of rosacea and postadolescent acne. Genuine infestations of the skin (scabies and pediculosis) and superficial skin infections (usually related to Staphylococcus aureus) were found more often in alcoholic vagrants than in non alcoholics and those with other psychiatric disorders. This also suggests that more specific alcoholrelated immune factors may be active. Depression in dermatological patients the concept of depression is frequently used to mean disillusion, disenchantment, helplessness, frustration or mental fatigue. True depressive illness is an important but frequently missed diagnosis for nonpsychiatrists. Up to onethird of medically ill patients have depressive symptoms and depression has a greater impact on mean health scores than angina, asthma or diabetes and more so when combined with chronic physical illness [1]. Depression, and to a lesser extent all forms of substance abuse, were the most overlooked diagnoses by dermatologists in 500 unselected dermatology patients examined by Musalek [3]. Screening for depressive diseases in patients with skin disease showed a prevalence of major depressive disorder in 8. Clinicians may underestimate the importance of depression believing that it is an almost inevitable reaction to a severe chronic skin condition. Item responses are scored 0 or 1 with a score over 2 being clinically significant. Clinicians need to be able to make a clear distinction between appropriate sadness in response to life events and a clinical depression. This is not to say that appropriate sadness should be dismissed or not addressed (for example, by suggesting opportunities for bereavement counselling or other support where suitable). Plus three or more of the following: 3 More than 5% weight loss in a month or persistent increase or decrease in appetitite. This is a chronic state of depression that may not be severe enough to meet the criteria for major depression. A depressed mood must be present for most of the day on most days for at least 2 years. The patient must not have gone more than 2 months without experiencing at least two of the following symptoms: 1 Poor appetite or overeating. Patients with chronic forms of depression are at risk of subsequent major depression, considerable social disability and unhealthy lifestyle choices such as poor diet, alcohol abuse and smoking. Depression in the elderly may be more manifested by irritability, selfneglect, somatic complaints or forgetfulness than conventional symptoms. In children, depression may be insidious and present as disruptive behaviour, irritability, truancy or somatic complaints [4]. A number of robust screening instruments [5] have been developed and validated to detect depression.
Canthaxanthin. Zanaflex.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96821
Pruritus Although some textbooks report an association with diabetes spasms prednisone discount 4 mg zanaflex, there are few detailed studies. A recent paper from Japan reported an increased prevalence of truncal pruritus compared with controls (11. Anogenital pruritus may be due to secondary infection with candidiasis or haemolytic streptococci [3]. This is a very broad group that is clinically characterized by hyperkeratosis or visible scaling or both. In many of them, distinct genetic defects can be elucidated revealing quite a few mechanisms and sometimes even pathways can be recognized, From a molecular perspective, it would be tempting to provide a classification based on molecular grounds, sorting out for instance keratinopathies relating to mutations in keratin genes from diseases relating to defects in lipid transport or cholesterol biosynthesis. Since this textbook is aimed primarily at dermatologists and physician scientists who have to make a clinical diagnosis and provide adequate management for their patients, the authors have decided to adhere to a classification scheme that is based on clinicogenetic and morphological features. It dates back more than 100 years and was first introduced by Peukert in 1899 [8]. Finally, this chapter will cover several cornification disorders that do not have a genetic basis, but are acquired or of unknown aetiology, It was coined at a time when the characteristics of human diseases were compared to those occurring in the animal kingdom. An important advance of the recent consensus conference on ichthyosis [4] was that we now differentiate between syndromic (Table 65. Instead, it is suggested to distinguish between common and rare forms of the disease. Specific pathophysiological aspects of all types of icthyoses are discussed with the respective entities. Generally, ichthyosis results in abnormal differentiation and/or abnormal desquamation showing for example impaired corneocyte shedding (retention hyperkeratosis) or accelerated keratinocyte production (epidermal hyperplasia/ hyperproliferative hyperkeratosis). The development of hyperkeratosis in these diseases may be understood as a homeostatic repair response aimed at compensating for an abnormal epidermal barrier [3,4]. A considerable number of patients indicate that they suffer from hypohidrosis and cannot perspire well [4]. Investigations Histology reveals orthohyperkeratosis with a diminished or absent granular layer.
Epidemiology Incidence and prevalence Riboflavin deficiency is endemic in populations whose diets rely heavily on unenriched cereals spasms of the bladder generic zanaflex 2 mg free shipping, or lack dairy products and meats. Age Riboflavin deficiency can occur at any age, though it may disproportionately affect schoolaged children, adolescents and the elderly. Clinical signs of chronic riboflavin deficiency include angular stomatitis, cheilitis, glossitis, dyssebacia of the nose and a seborrhoeic dermatitislike eruption. Angular stomatitis initially presents with small papules at the corners of the mouth, which subsequently extend laterally, macerate, fissure and bleed. Glossitis is characterized by prominent lingual papillae early on, with transition to a smooth magentacoloured tongue over time. Riboflavin deficiency dermatitis commonly involves the nasolabial folds, nasal ala, nasal bridge, forehead, cheeks and postauricular regions. It is worse in areas of trauma and chafing, thus making it prominent in the inguinal folds and perineum of infants and in individuals who perform heavy physical activity [75]. Differential diagnosis Ethnicity There is no ethnic predilection for riboflavin deficiency. Associated diseases Studies suggest that riboflavin deficiency may be associated with increased plasma homocysteine levels, impaired iron handling and anaemia, cardiovascular disease, night blindness, developmental abnormalities, peripheral neuropathy and cancer [70]. Disease course and prognosis Riboflavin deficiency carries an excellent prognosis with striking response to riboflavin supplementation. Pathophysiology Predisposing factors Riboflavin deficiency may develop as a result of decreased dietary intake, malabsorption and phototherapy. Adolescents, the elderly, alcoholics and individuals with eating disorders are at risk for inadequate nutritional intake. Breastfed infants of riboflavindeficient mothers, as well as infants weaned to non milk products, are also at risk. Impaired absorption of riboflavin has been associated with bariatric surgery and the use of various medications, including chlorpromazine or other tricyclics [71,72]. Borate can complex with riboflavin, increase urinary excretion of riboflavin and inhibit riboflavindependent enzymes [73]. Finally, phototherapy for neonatal hyperbilirubinaemia causes photodecomposition of riboflavin [74].

The hair cuticle is formed initially as a single cell layer spasms hand order zanaflex 4 mg with mastercard, but the cells become progressively imbricated (tilelike) as they move periph erally. The cells become flattened, first in a direction at right angles to the plane of the follicle, and then becoming progressively angu lated so that the outer edges of the cells point in an upward direc tion. The cuticle has important protective properties: it acts as a barrier to physical and chemical insults, and also maintains the integrity of the hair shaft. Eventually this process may lead to exposure of the cortex and fracture of the hair shaft. Cells destined to form the cortex gradually become more fusiform in shape as they migrate upwards from the hair bulb. Keratin filaments are crosslinked to keratinassociated proteins, which form a matrix between the fil aments. Pigment granules that are normally dispersed throughout the cortex are not included. The medulla is a variable structure in human hairs, where it may be continuous, discontinuous or absent. Largediameter hairs are more likely to contain a medulla, although the relation ship between hair diameter and medullation is not clearcut. A plexus of longitudinally aligned sensory nerve fibres surrounds the isthmus region. Small nerve fibres may also be arranged in a circular fashion outside the longitudinal fibres. Several different types of nerve endings are found around human hair follicles, including free nerve endings, piloRuffini nerve end ings and Merkel nerve endings [35,36]. In other species, lamellated nerve endings are found in richly innervated sinus hair follicles. The relatively translucent filaments, set in a more dense sulphurrich matrix, appear as concentric lamellae (macrofibrils), giving a characteristic fingerprint pattern. The period of active hair growth is known as anagen and the duration of this phase is responsible for determining the final length of the hair. In most hair follicles in most animals, anagen is relatively brief, lasting a few weeks at most. The entry of a resting hair follicle into anagen is heralded by the onset of mitotic activity in epithelial cells overlying the dermal papilla at the base of the follicle (the secondary epithelial germ). In most follicle types (vibrissae follicles are an exception), the lower part of the follicle elongates downwards along a preformed der mal tract (the stele). The dermal papilla expands from a tightly packed ball of cells into a flask shaped structure where the cells become separated by an extra cellular matrix rich in proteoglycans and basement membrane proteins. A network of capillary blood vessels develops around the lengthening follicle, extending into the dermal papilla in larger follicles.
Blisters are typically symmetrically distributed and may persist for several days muscle relaxant potency buy cheap zanaflex 2 mg. After mechanical irritation erosions and yellowish or haemorrhagic crusts develop. The mucosae of the eyes, nose, pharynx, oesophagus and anogenital areas are rarely affected (reviewed in [175,176]). Some forms such as prurigolike, papular, eczematous, vesicular and erythrodermic pemphigoid may later develop tense blisters and transform into the classical type. Multiple cases with a close association with preceding vaccinations were reported, most of them in infants. Due to the high rate of vaccinations in this age group, a causative relation is difficult to confirm. In infants, the distribution of the lesions is often acral, in particular palmar and plantar [41]. For treatment, systemic corticosteroids are usually combined with dapsone or sulfapyridine [194]. The index records severity of: (i) skin lesions separately for classical lesions, i. In brief, diseases of the pemphigus group can be easily differentiated on the basis of distinctive clinical (positive Nikolsky sign) and immunopathological features. Eczema, erosions and tense blisters restricted to the site of percutaneous endoscopic gastrostomy (c). Mortality varies considerably between different populations (outpatients versus inpatients, different countries, secondary or tertiary referral centres), and treatments. Risk factors for lethal outcome are old age (greater than 80 years), extensive disease, high doses of prednisolone (>35 mg/day), serum albumin levels of less than 3. If these investigations are negative, other diagnoses may be considered (see Differential diagnosis). Disseminated tense blisters, erosions and crusts on the lower abdomen, genitalia and lower extremities in an infant (a). Generalized erythema, numerous tense vesicles and some erosions on the back of a 3yearold boy (b). About 90% of patients can be diagnosed based on the clinical picture and serological tests. Antilaminin 332 pemphigoid Epidermolysis bullosa acquisita Anti-p200/ laminin g1 pemphigoid Topical and systemic steroids are the mainstay of treatment.
Porgan, 25 years: At the lower tip of the hair bulb it consists of a single layer of cuboidal cells, becoming multilayered in the region of the upper hair bulb. Clinical features Maffucci syndrome belongs to the spectrum of enchondromatoses [121�123].
Miguel, 64 years: Facial hair in boys first appears at about the same time as the axillary hair, starting at the corners of the upper lip, and spreading medially to complete the moustache and then the cheeks and beard. Kashin�Beck disease describes selenium deficiency with predominantly bony disease.
Jack, 29 years: The trichogram analysis of a hair pluck sample usually shows more than 25% of telogen hairs in acute telogen effluvium [1]. Associated diseases Acquired pernicious anaemia is an autoimmune gastritis characterized by destruction of gastric parietal cells and loss of intrinsic factor.
Ines, 58 years: Associated diseases Recent studies suggest that vitamin D sufficiency may be protective against musculoskeletal disease, infection, autoimmune disease, cardiovascular disease, diabetes, neurocognitive dysfunction, various common cancers, infertility and adverse pregnancy/birth outcomes [23,24]. Clinical features History Porokeratoses present with single or multiple papules or plaques which develop into annular lesions with a thin raised border.
Kaffu, 40 years: Patients are more often passive than aggressive, even though they have a widespread disfigurement. Enchondromas may degenerate into chondrosarcomas, and differentiation may be difficult.
References